UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM
(Mark One)
For the fiscal year ended
or
For the transition period from __________ to __________
Commission File Number
(Exact name of registrant as specified in its charter)
| (State or other jurisdiction of incorporation or organization) | (I.R.S. Employer Identification No.) |
|
|
( |
| (Address of principal executive offices) | (Registrant’s telephone number, including area code) |
Securities registered pursuant to Section 12(b) of the Act:
| Title of each class | Trading symbol(s) | Name of each exchange on which registered |
|
The (Nasdaq Capital Market) |
Indicate by check mark if the registrant is a
well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ☐
Indicate by check mark if the registrant is not
required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ☐
Indicate by check mark whether the registrant
(1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months
(or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements
for the past 90 days.
Indicate by check mark whether the registrant
has submitted electronically every Interactive Data File required to be submitted pursuant to Rule 405 of Regulation S-T (§ 232.405)
during the precedent 12 months (or for such shorter period that the registrant was required to submit such files).
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company or an emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company” and “emerging growth company” in Rule 12b-2 of the Exchange Act.
| Large accelerated filer | ☐ | Accelerated filer | ☐ | |||
| ☒ | Smaller reporting company | |||||
| Emerging growth company |
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Indicate by check mark whether the registrant
is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes ☐
State the aggregate market value of the voting
and non-voting common equity held by non-affiliates computed by reference to the price at which the common equity was last sold, or the
average bid and asked price of such common equity, as of October 31, 2021: $
As of July 28, 2022, the registrant had outstanding shares of common stock.
DOCUMENTS INCORPORATED BY REFERENCE
None.
TABLE OF CONTENTS
| ii |
Cautionary Note Regarding Forward-Looking Statements
This Report on Form 10-K (“Report”) includes “forward-looking statements” within the meaning of the federal securities laws. All statements other than statements of historical fact are “forward-looking statements” for purposes of this Report, including any projections of earnings, revenue or other financial items, any statements regarding the plans and objectives of management for future operations, any statements concerning proposed new products or services, any statements regarding future economic conditions or performance, any statements regarding expected benefits from any transactions and any statements of assumptions underlying any of the foregoing. In some cases, forward-looking statements can be identified by use of terminology such as “may,” “will,” “should,” “believes,” “intends,” “expects,” “plans,” “anticipates,” “estimates,” “goal,” “aim,” “potential” or “continue,” or the negative thereof or other comparable terminology. Although we believe that the expectations reflected in the forward-looking statements contained in this Report are reasonable, there can be no assurance that such expectations or any of the forward-looking statements will prove to be correct, and actual results could differ materially from those projected or assumed in the forward-looking statements. Thus, investors should refer to and carefully review information in future documents we file with the U.S. Securities and Exchange Commission (“Commission”). Our future financial condition and results of operations, as well as any forward-looking statements, are subject to inherent risk and uncertainties, including, but not limited to, the risk factors set forth in “Part I, Item 1A – Risk Factors” set forth in this Report and for the reasons described elsewhere in this Report. Among others, these include our estimates regarding expenses, future revenues, capital requirements and needs for additional financing; whether the United States Food and Drug Administration (“FDA”) approves our Investigational New Drug Application (“IND”) after we complete the FDA’s requested studies and submit a response to the FDA’s clinical hold, so that we can commence our planned clinical trial involving locally advanced, inoperable, non-metastatic pancreatic cancer (“LAPC”); the success and timing of our preclinical studies and clinical trials; the potential that results of preclinical studies and clinical trials may indicate that any of our technologies and product candidates are unsafe or ineffective; our dependence on third parties in the conduct of our preclinical studies and clinical trials; the difficulties and expenses associated with obtaining and maintaining regulatory approval of our product candidates; the material adverse impact that the coronavirus pandemic may have on our business, including our planned clinical trial involving LAPC, which could materially affect our operations as well as the business or operations of third parties with whom we conduct business; and whether the FDA will approve our product candidates after our clinical trials are completed, assuming the FDA allows our clinical trials to proceed after submission and review of our response to the FDA’s clinical hold. All forward- looking statements and reasons why results may differ included in this Report are made as of the date hereof, and we do not intend to update any forward-looking statements except as required by law or applicable regulations. Except where the context otherwise requires, in this Report, the “Company,” “we,” “us” and “our” refer to PharmaCyte Biotech, Inc., a Nevada corporation, and, where appropriate, its subsidiaries.
| iii |
PART I
ITEM 1. BUSINESS.
Product Candidates
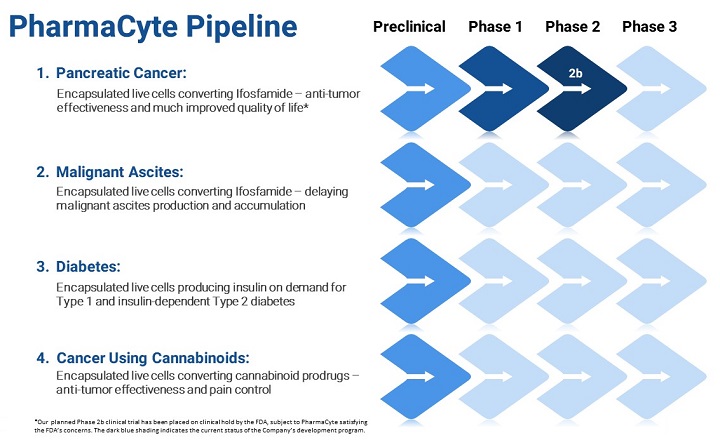
We are a biotechnology company focused on developing cellular therapies for cancer, diabetes, and malignant ascites based upon a proprietary cellulose-based live cell encapsulation technology known as “Cell-in-a-Box®..” The Cell-in-a-Box® technology is intended to be used as a platform upon which therapies for several types of cancer, including LAPC, will be developed. The current generation of our product candidate is referred to as “CypCaps™.”
The Cell-in-a-Box® encapsulation technology potentially enables genetically engineered live human cells to be used to produce various biologically -active molecules. The technology is intended to result in the formation of pinhead -sized cellulose-based porous capsules in which genetically modified live human cells can be encapsulated and maintained. In a laboratory setting, this proprietary live cell encapsulation technology has been shown to create a micro-environment in which encapsulated cells survive and flourish. They are protected from environmental challenges, such as the sheer forces associated with bioreactors and passage through catheters and needles, etc., which we believe enables greater growth and production. The capsules are largely composed of cellulose (cotton) and are bio inert.
We are developing therapies for pancreatic and other solid cancerous tumors by using genetically engineered live human cells that we believe are capable of converting a cancer prodrug into its cancer-killing form. We encapsulate those cells using the Cell-in-a-Box® technology and place those capsules in the body as close as possible to the tumor. In this way, we believe that when a cancer prodrug is administered to a patient with a particular type of cancer that may be affected by the prodrug, the killing of the patient’s cancerous tumor may be optimized.
We are also developing a way to delay the production and accumulation of malignant ascites that results from many types of abdominal cancerous tumors. Our potential therapy for malignant ascites involves using the same encapsulated cells we employ for pancreatic cancer but placing the encapsulated cells in the peritoneal cavity of a patient and administering ifosfamide intravenously.
We have also been developing a potential therapy for Type 1 diabetes and insulin-dependent Type 2 diabetes. Our product candidate for the treatment of diabetes consists of encapsulated genetically modified insulin-producing cells. The encapsulation will be done using the Cell-in-a-Box® technology. Implanting these encapsulated cells in the body is designed to have them function as a bio-artificial pancreas for purposes of insulin production.
In addition to the two cancer programs discussed above, we have been working on ways to exploit the benefits of the Cell-in-a-Box® technology to develop therapies for cancer that involve prodrugs based upon certain constituents of the Cannabis plant. However, until the FDA allows us to commence our clinical trial in LAPC and we are able to validate our Cell-in-a-Box® encapsulation technology in a clinical trial, we are not spending any further resources developing our Cannabis Program.
| 1 |
Cancer Therapy
Targeted Chemotherapy
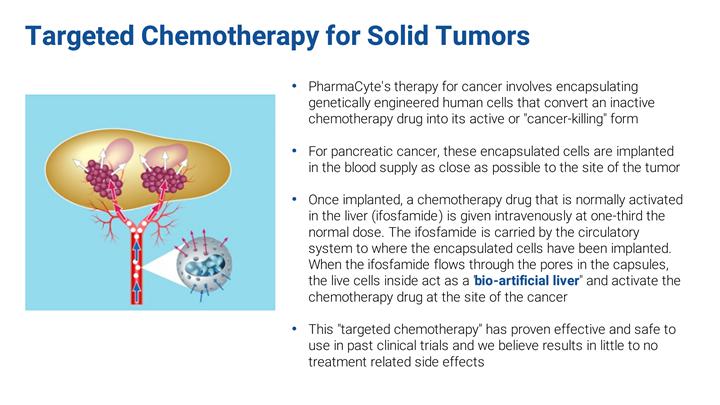
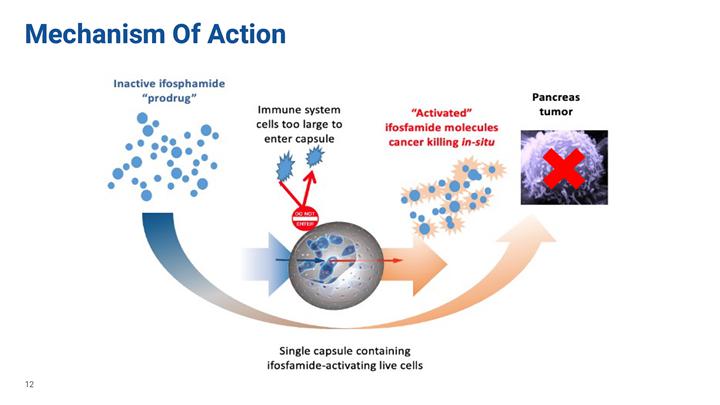
Our therapy for cancer involves encapsulating genetically engineered human cells that convert an inactive chemotherapy drug into its active or “cancer-killing” form. For pancreatic cancer, these encapsulated cells are implanted in the blood supply to the patient’s tumor as close as possible to the site of the tumor. Once implanted, a chemotherapy drug that is normally activated in the liver (ifosfamide) is given intravenously at one-third the normal dose. The ifosfamide is carried by the circulatory system to where the encapsulated cells have been implanted. When the ifosfamide flows through pores in the capsules, the live cells inside act as a “bio-artificial liver” and activate the chemotherapy drug at the site of the cancer.
| 2 |
| 3 |

Pancreatic Cancer
| 4 |
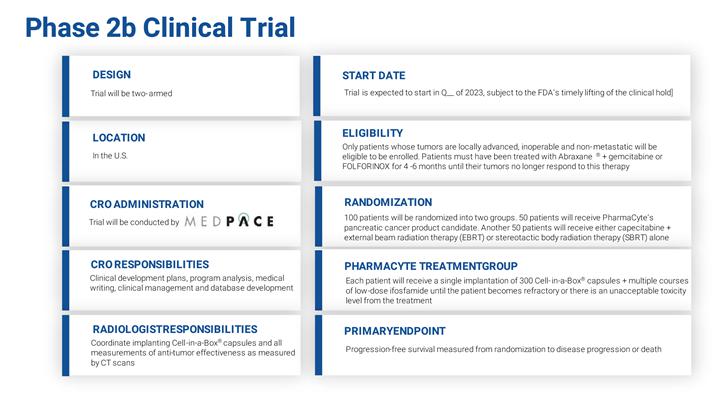
We believe an unmet medical need exists for patients with LAPC whose pancreas tumor no longer responds after 4-6 months of treatment with either Abraxane® plus gemcitabine or the 4-drug combination known as FOLFIRINOX. Both combinations are the current standards of care for pancreatic cancer. We believe that these refractory patients have no effective treatment alternative once their tumors no longer respond to these therapies. Treatments are being tried at various cancer centers in the U.S. in an attempt to address this lack of an effective treatment for LAPC patients, but their success is far from certain.
Two of the most commonly used treatments for these patients are 5-fluorouracil (“5-FU”) or capecitabine (a prodrug of 5-FU) plus radiation (chemoradiation therapy). More recently, radiation treatment alone is being used at some cancer centers in the U.S.
We believe that these treatments are only marginally effective in treating the LAPC tumor and result in serious side effects.
We believe that our therapy for LAPC, if approved, can serve as a “consolidation therapy” that can be used with the current standards of care and thus address this critical unmet medical need. On September 1, 2020, we submitted an Investigational New Drug Application (“IND”) to the FDA for a planned Phase 2b clinical trial in LAPC. Highlights of our planned clinical trial are shown below:
| 5 |
Clinical Hold
On October 1, 2020, we received notice from the FDA that it had placed our IND on clinical hold. On October 30, 2020, the FDA sent us a letter setting forth the reasons for the clinical hold and providing specific guidance on what we must do to have the clinical hold lifted.
In order to address the clinical hold, the FDA has requested that we:
| · | Provide additional sequencing data and genetic stability studies; |
| · | Conduct a stability study on our final formulated product candidate as well as the cells from our Master Cell Bank (“MCB”); |
| · | Evaluate the compatibility of the delivery devices (the prefilled syringe and the microcatheter used to implant the CypCaps™) with our product candidate for pancreatic cancer; |
| · | Provide additional detailed description of the manufacturing process of our product candidate for pancreatic cancer; |
| · | Provide additional product release specifications for our encapsulated cells; |
| · | Demonstrate comparability between the 1st and 2nd generation of our product candidate for pancreatic cancer and ensure adequate and consistent product performance and safety between the two generations; |
| · | Conduct a biocompatibility assessment using the capsules material; |
| · | Address specified insufficiencies in the Chemistry, Manufacturing and Controls information in the cross-referenced Drug Master File; |
| · | Conduct an additional nonclinical study in a large animal (such as a pig) to assess the safety, activity, and distribution of the product candidate for pancreatic cancer; and |
| · | Revise the Investigators Brochure to include any additional preclinical studies conducted in response to the clinical hold and remove any statements not supported by the data we generated. |
The FDA also requested that we address the following issues as an amendment to our IND:
| · | Provide a Certificate of Analysis for pc3/2B1 plasmid that includes tests for assessing purity, safety, and potency; |
| · | Perform qualification studies for the drug substance filling step to ensure that the product candidate for pancreatic cancer remains sterile and stable during the filling process; |
| · | Submit an updated batch analysis for the product candidate for the specific lot that will be used for manufacturing all future product candidates; |
| · | Provide additional details for the methodology for the Resorufin (CYP2B1) potency and the PrestoBlue cell metabolic assays; |
| · | Provide a few examples of common microcatheters that fit the specifications in our Angiography Procedure Manual; |
| · | Clarify the language in our Pharmacy Manual regarding proper use of the syringe fill with the product candidate for pancreatic cancer; and |
| · | Provide a discussion with data for trial of the potential for cellular and humoral immune reactivity against the heterologous rat CYP2B1 protein and potential for induction of autoimmune-mediated toxicities in our study population. |
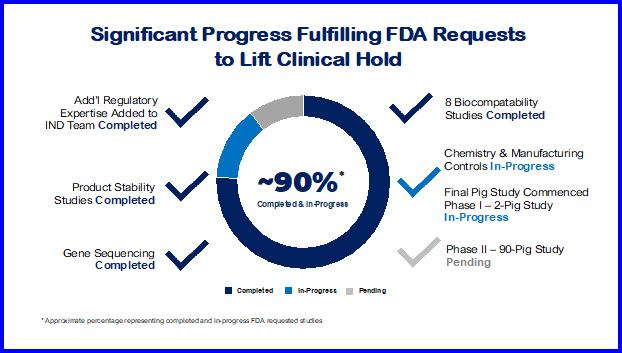
We assembled a scientific and regulatory team of experts to address the FDA requests. That team has been working diligently to complete the items requested by the FDA. To date we believe we have made significant progress in fulfilling the FDA requests needed to lift the clinical hold.
| 6 |
The following provides a detailed summary of our activities to have the clinical hold lifted:
| · | Additional Regulatory Expertise Added to IND Team. In addition to our existing team of regulatory experts, we retained Biologics Consulting to perform a regulatory “Gap Analysis” and to assist us with our resubmission of the IND. Biologics Consulting is a full-service regulatory and product development consulting firm for biologics, pharmaceuticals and medical devices and has personnel with extensive FDA experience. |
| · | Stability Studies on Our Clinical Trial Product Candidate for Pancreatic Cancer. We have successfully completed the required product stability studies. The timepoints were 3, 6, 9, 12, 18 and 24-months of our product candidate for pancreatic cancer being stored frozen at -80C. These studies included container closure integrity testing for certain timepoints. |
| · | Additional Studies Requested by the FDA. We have successfully completed various additional studies requested by the FDA, including a stability study on the cells from our MCB used to make our CypCaps™. We are already at the 36-month stability timepoint for the cells from our MCB. We are also collating existing information on the reproducibility and quality of the filling of the MCB cells into vials ready for CypCaps™ manufacturing. |
| · | Determination of the Exact Sequence of the Cytochrome P450 2B1 Gene. We have completed the determination of the exact sequence of the cytochrome P450 2B1 gene inserted at the site previously identified on chromosome 9 using state-of-the-art nanopore sequencing. This is a cutting edge, unique and scalable technology that permits real-time analysis of long DNA fragments. The result of this analysis of the sequence data confirmed that the genes are intact. |
| 7 |
| · | Confirmation of the Exact Sequence of the Cytochrome P450 2B1 Gene Insert. An additional, more finely detailed, analysis of the integration site of the cytochrome P450 2B1 gene from the augmented HEK293 cell clone that is used in our CypCaps™ was found to be intact. In this new study, we were able to confirm the previously determined structure of the integrated transgene sequence using more data points. These studies also set the stage for a next step analysis to determine the genetic stability of the cytochrome P450 2B1 gene at the DNA level after multiple rounds of cell growth. This new study has been completed in which our original Research Cell Bank (“RCB”) cells were compared with cells from the MCB. The analysis confirmed that the cytochrome P450 2B1 and the surrounding sequence has remained stable with no changes detected at the DNA level. |
|
|
· |
Biocompatibility Studies. We have been involved with 10 biocompatibility studies requested by the FDA, 8 of which have been completed successfully. The remaining studies are underway or about to start. The Acute Systemic Toxicity Study of Empty Cellulose Sulphate Capsules in Mice is underway. The Skin Sensitization Study of Empty Cellulose Sulphate Capsules in Guinea Pigs is about to start. These last two studies should be completed well before the pig study (see below) is completed.
To enable the biocompatibility studies to be performed, we had Austrianova Singapore Pte. Ltd. (“Austrianova”) manufacture an additional 400 syringes of empty capsules.
Systemic Toxicity Testing. We evaluated the potential toxicity of the capsule component of our product candidate for pancreatic cancer and determined there is no evidence of toxicity in any of the parameters examined. The study also confirmed previous data that shows our capsule material is bioinert. |
| · | Micro-Compression and Swelling Testing. This testing is underway. We are developing and optimizing two reproducible methods for testing and confirming the physical stability and integrity of our CypCaps™ under extreme pressure. These studies required the acquisition of new equipment by Austrianova as well as validation and integration into Austrianova’s Quality Control laboratory. |
| · | Break Force and Glide Testing. We are in the process of developing a protocol to measure whether the syringe, attached to the catheter when used to expel the capsules, will still have a break and glide force that is within the specifications we have established. We are setting the specifications based on the syringe/plunger manufacturer’s measured break and glide forces, or alternatively, accepted ranges for glide forces routinely used in the clinic. |
| · | Capsules Compatibility with the Syringe and Other Components of the Microcatheter Delivery System. We are in the process of showing that CypCaps™ are not in any way adversely affected by the catheters used by interventional radiologists to deliver them into a patient. Compatibility data is being generated to demonstrate that the quality of the CypCaps™ is maintained after passage through the planned microcatheter systems. |
| · | CypCaps Capsules and Cell Viability after Exposure to Contrast Medium. We have commenced testing to show that exposure of CypCaps™ to the contrast medium interventional radiologists used to implant the CypCaps™ in a patient has no adverse effect on CypCaps™. Contrast medium is used to visualize the blood vessels during implantation. |
| · | Master Drug File Information. Austrianova is providing additional detailed confidential information on the manufacturing process, including information on the improvements and advancements made to our product candidate for pancreatic cancer since the last clinical trials were conducted with respect to reproducibility and safety. However, Austrianova has not changed the overall physical characteristics of CypCaps™ between the 1st and 2nd generations. We are supporting Austrianova financially with this work. |
| · | Additional Documentation Requested by the FDA. We are in the process of updating our IND submission documentation, including our discussion on immunological aspects of our treatment for LAPC. |
| · | Pig Study. We have commenced a study in pigs to address biocompatibility and long-term implantation and dispersion of CypCaps™. The study has two phases: (i) a pilot study with 2 pigs; and (ii) a 90-pig study. The first phase has commenced. We believe this study should complement the positive data already available from the previous human clinical trials showing the safety of CypCaps™ implantation in human patients. On July 21, 2022, the first phase of the pig study commenced. The second phase of the pig study may be delayed as a result of supply chain problems, including production delays at Austrianova possibly related to their financial condition. |
| 8 |
Malignant Ascites

| 9 |
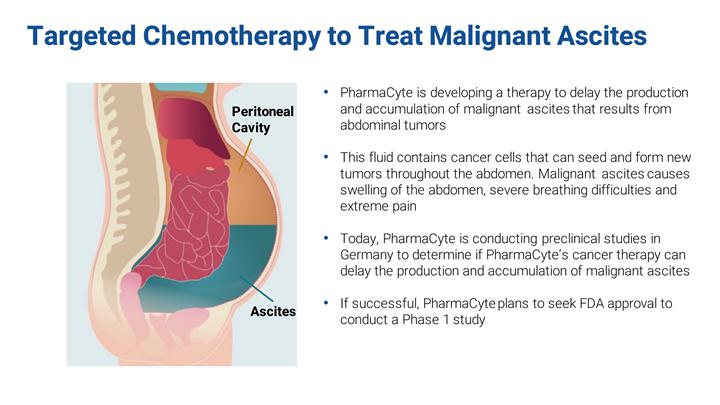
We have been exploring ways to delay the production and accumulation of malignant ascites that results from several types of abdominal tumors. Malignant ascites is a fluid that is secreted by an abdominal tumor into the abdomen after the tumor reaches a certain stage of growth. This fluid contains cancer cells that can seed and form new tumors throughout the abdomen. As this malignant ascites fluid accumulates in the abdominal cavity, it can cause gross swelling of the abdomen, severe breathing difficulties and extreme pain. Accumulated malignant ascites must be removed by paracentesis on a periodic basis. This procedure is painful and costly. We know of no available therapy that prevents or delays the production and accumulation of malignant ascites. Seven preclinical studies were conducted by Translational Drug Development (“TD2”), an early-stage clinical research organization (“CRO”) specializing in oncology, to determine whether the combination of Cell-in-a-Box® encapsulated cells plus low doses of ifosfamide could delay the production and accumulation of malignant ascites. The data from these studies suggested that our cancer therapy might play a role in malignant ascites fluid production and accumulation. However, the data were difficult to interpret with certainty.
On May 23, 2022, we initiated the first in a new series of studies to test the ability of our pancreatic cancer therapy to treat malignant ascites. This is the eighth and final preclinical study that may lead to a Phase 1 clinical trial. Such a clinical trial may allow us to validate the Cell-in-a-Box® technology much faster than our planned Phase 2b clinical trial in LAPC.
If this new series of studies is successful, we plan to submit an IND to seek approval from the FDA to conduct a Phase 1 clinical trial to determine if our product candidate for pancreatic cancer can delay the production and accumulation of malignant ascites.
Diabetes Therapy

| 10 |
A Bio-Artificial Pancreas to Treat Diabetes
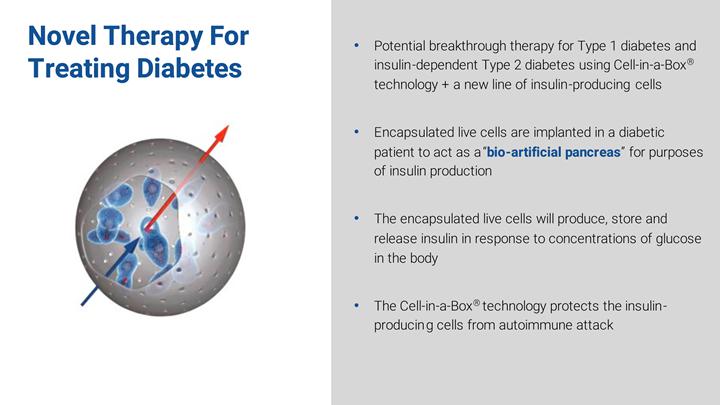
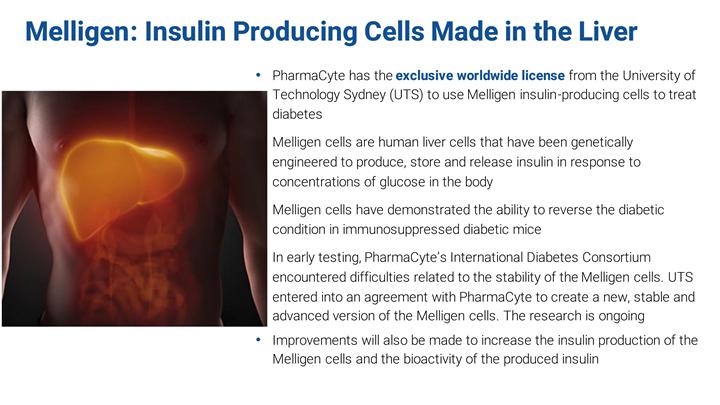
We are developing a therapy for Type 1 diabetes and insulin-dependent Type 2 diabetes based upon the encapsulation of a human cell line genetically engineered to produce, store and release insulin at levels in proportion to the levels of blood sugar in the human body.
The cell line we select will be encapsulated using the Cell-in-a-Box® encapsulation technology.
If appropriate animal testing is completed successfully, we intend to submit an IND to the FDA to seek its approval to transplant encapsulated insulin-producing cells into diabetic patients. The goal for this approach is to develop a bio-artificial pancreas for purposes of insulin production for diabetic patients who are insulin-dependent.
| 11 |
Our diabetes program began with two of the most critical components of a biological diabetes therapy - a line of human cells which release insulin in response to the blood glucose level in their environment and a technology to protect the cells from an attack by the immune system once they are transplanted into a patient to replace his or her own destroyed insulin-producing cells. This technology is the Cell-in-a-Box® encapsulation technology. The cells we initially used are Melligen cells. They are patent-protected and have been licensed to us by University of Technology Sydney (“UTS”).
Putting Melligen cells and the Cell-in-a-Box® technology together, we conducted the first functional study in diabetic mice. The results did not meet our expectations. We discovered that, contrary to what we had expected and what we had read in published scientific papers on the Melligen cells published by UTS, the cells are not stable. With extensive testing and experiments, we discovered that the Melligen cells lose some of their specific beneficial properties over time.
We entered into a research agreement with UTS to create an advanced version of the Melligen cells for the treatment of diabetes. Under this agreement, improvements are to be made to the Melligen cells that we believe will increase their stability, increase their insulin production and increase the bioactivity of the produced insulin.
Until recently, UTS has been conducting this research. The work is being funded by us and UTS. Our portion of the funding was previously paid to UTS. The research to date has not produced the results we had anticipated and is taking longer than we anticipated. It remains to be seen whether the Melligen cells are capable of producing the required insulin to be a viable cell line for the treatment of diabetes. Further research is requied.
Meanwhile, we have been working with two internationally renowned academic institutions to develop a cell line that will form the backbone of our Diabetes Program. These institutions are developing a stem-cell derived beta islet cell that we plan to encapsulate to treat Type 1 and insulin-dependent Type 2 diabetes. We are currently negotiating agreements with these institutions, although no assurance can be give that the negotiations will be successful.
| 12 |
Cannabinoids to Treat Cancer

| 13 |
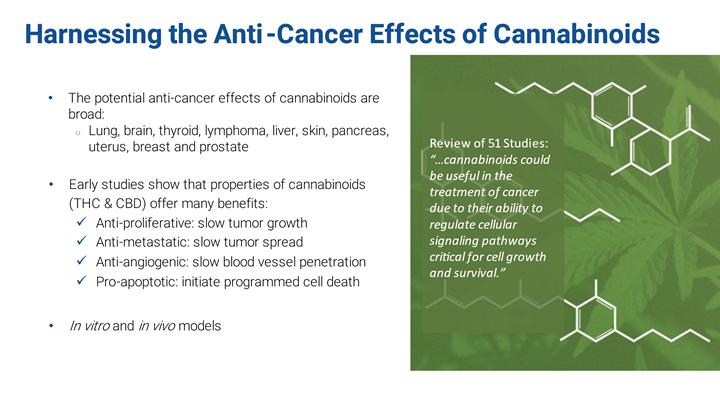
Numerous studies have demonstrated the therapeutic potential of certain cannabinoids in patients with cancer. Studies have shown that cannabinoids are potentially: (i) anti-proliferative (slow tumor growth); (ii) anti-metastatic (slow tumor spread); (iii) anti-angiogenic (slowing blood vessel development); and (iv) pro-apoptotic initiate programed cell death). In in vitro and in vivo models, the therapeutic potential of cannabinoids is broad. Results support the therapeutic potential in lung, brain, thyroid, lymphoma, liver, skin, pancreas, uterus breast and prostate cancers.
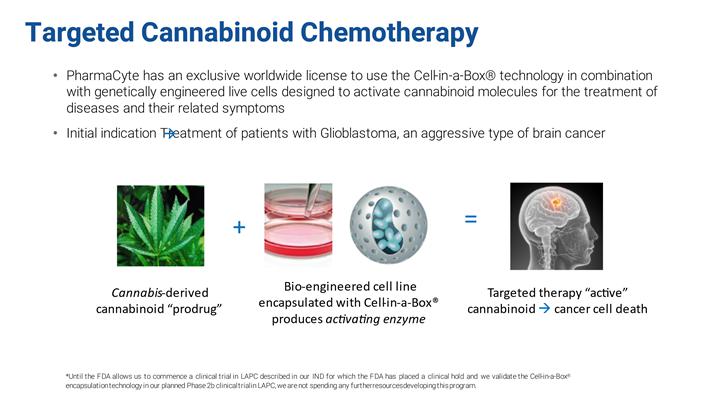
We intend to use the Cell-in-a-Box® technology in combination with genetically modified cell lines designed to activate cannabinoid molecules for the treatment of diseases and their related symptoms. Our initial target will be glioblastoma – a very difficult-to treat form of brain cancer. However, until the FDA allows us to commence our clinical trial in LAPC and we are able to validate our Cell-in-a-Box® encapsulation technology in a clinical trial, we are not spending any further resources developing our Cannabis Program.
| 14 |
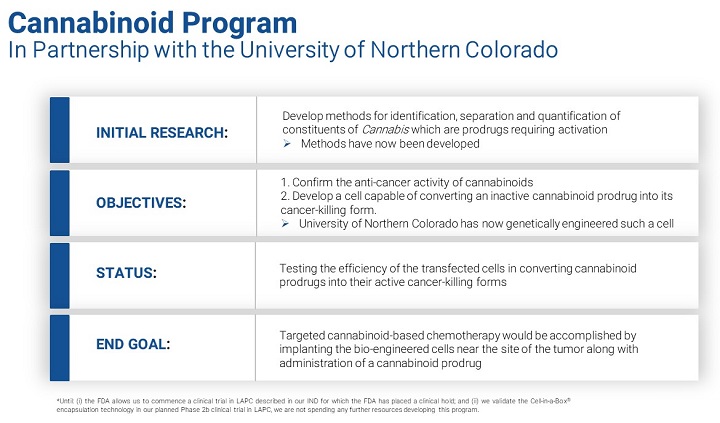
The goal of the original research was to develop methods for the identification, separation and quantification of constituents of Cannabis, some of which are prodrugs, which could potentially be used in combination with the Cell-in-a-Box® technology to treat cancer. After achieving this milestone, we then went on to assess the synthesis of the patG gene and its incorporation into a vector, transfection of human embryonic kidney cells using this vector and assessment of cannabinoic acid decarboxylase activity. We later identified an organism whose genome contains the genetic code for production of an enzyme capable of activating a cannabinoid prodrug into its active cancer-killing form.
Our Cannabis Program now has two primary areas of focus. The first is evaluating the therapeutic potential of cannabinoids in our main “target” tumor – glioblastoma. In laboratory research, we have confirmed that a purified cannabinoid showed a potent dose-dependent decrease in cell viability for various cancers, suggesting that this cannabinoid exhibits significant anti-proliferative effects (stops the growth and multiplication of cancer cells). This activity has been demonstrated in brain, pancreas, breast, lung, colon and melanoma cancer cells. The second area of focus is in finding an enzyme capable of converting an inactive, side-effect-free, cannabinoid prodrug into its active cancer-killing form.
Clinically, targeted cannabinoid-based chemotherapy would be accomplished by implanting the encapsulated bio-engineered cells near the site of a tumor, along with administration of a cannabinoid prodrug which would become activated at the site of the tumor by an enzyme produced by the encapsulated cells. We believe this could lead to better efficacy than existing therapies with minimal treatment related adverse events.
Impact of the COVID-19 Pandemic on Operations
The coronavirus SARS-Cov2 pandemic (“COVID-19”) continues to cause uncertainty and significant, industry-wide delays in clinical trials. The availability of vaccines holds promise for the future; however, new variants of the virus and potential waning immunity from vaccines may result in continued impact from COVID-19 in the future, which could adversely impact our operations. Although we are not yet in a clinical trial, we have filed an IND with the FDA to commence a clinical trial in LAPC. While the IND has been placed on clinical hold by the FDA, we have assessed the impact of COVID-19 on our operations.
As of the date of this Report, COVID-19 has had an impact upon our operations and that impact is increasing. The impact relates to, among other things, delays in (i) completing studies required by the FDA; (ii) manufacturing a new batch of CypCap™ for our planned clinical trial in LAPC; (iii) manufacturing syringes of CypCaps™ for use in our Malignant Ascites Program; (iv) securing third party contractors to conduct various research and development projects; and (v) disruptions in our supply chain.
As a result of COVID-19, commencement of our planned clinical trial to treat LAPC may be delayed beyond lifting of the clinical hold by the FDA should that occur. Also, enrollment may be difficult for the reasons discussed above. In addition, after enrollment in the trial, if a patient contracts COVID-19 during his or her participation in the trial or is subject to isolation or shelter in place restrictions, this may cause him or her to drop out of our clinical trial, miss scheduled therapy appointments or follow-up visits or otherwise fail to follow the clinical trial protocol. If a patient is unable to follow the clinical trial protocol or if the trial results are otherwise affected by the consequences of COVID-19 on patient participation or actions taken to mitigate COVID-19 spread, the integrity of data from the clinical trial may be compromised or not be accepted by the FDA. This could further adversely impact or delay our clinical development program if the FDA allows it to proceed.
Clinical trials in the biopharma industry may be delayed due to COVID-19. There are numerous reasons for these potential delays. For example, patients have shown a reluctance to enroll or continue in a clinical trial due to fear of exposure to COVID-19 when they are in a hospital or doctor’s office. There are local, regional, and state-wide orders and regulations restricting usual normal activity by people. These discourage and interfere with patient visits to a doctor’s office if the visit is not COVID-19 related. Healthcare providers and health systems are shifting their resources away from clinical trials toward the care of COVID-19 patients. The FDA and other healthcare providers are making product candidates for the treatment of COVID-19 a priority over product candidates unrelated to COVID-19.
It is highly speculative in projecting the effects of COVID-19 on our proposed clinical development program and our company generally. The effects of COVID-19 may quickly and dramatically change over time. Its evolution is difficult to predict, and no one can say with certainty when the pandemic will fully subside.
| 15 |
History of the Business
In 2013, we restructured our operations to focus on biotechnology. On January 6, 2015, we changed our name from “Nuvilex, Inc.” to “PharmaCyte Biotech, Inc.” to reflect the nature of our business.
We are a biotechnology company focused on developing and preparing to commercialize cellular therapies for cancer, diabetes, and malignant ascites using our live cell encapsulation technology. This resulted from entering into the following agreements.
Commencing in May 2011, we entered into a series of agreements and amendments with SG Austria Pte. Ltd. (“SG Austria”) to acquire certain assets from SG Austria as well as an exclusive, worldwide license to use, with a right to sublicense, the Cell-in-a-Box® technology and trademark for the development of therapies for cancer (“SG Austria APA”).
In June 2013, we and SG Austria entered a Third Addendum to the SG Austria APA (“Third Addendum”). The Third Addendum materially changed the transaction contemplated by the SG Austria APA. Under the Third Addendum, we acquired 100% of the equity interests in Bio Blue Bird and received a 14.5% equity interest in SG Austria. We paid: (i) $500,000 to retire all outstanding debt of Bio Blue Bird; and (ii) $1.0 million to SG Austria. We also paid SG Austria $1,572,193 in exchange for a 14.5% equity interest of SG Austria. The transaction required SG Austria to return to us the 66,667 shares of our common stock held by SG Austria and for us to return to SG Austria the 67 shares of common stock of Austrianova we held.
Effective as of the same date we entered the Third Addendum, we and SG Austria also entered a Clarification Agreement to the Third Addendum (“Clarification Agreement”) to clarify and include certain language that was inadvertently left out of the Third Addendum. Among other things, the Clarification Agreement confirmed that the Third Addendum granted us an exclusive, worldwide license to use, with a right to sublicense, the Cell-in-a-Box® technology and trademark for the development of therapies for cancer.
With respect to Bio Blue Bird, Bavarian Nordic A/S (“Bavarian Nordic”) and GSF-Forschungszentrum für Umwelt u. Gesundheit GmbH (collectively, “Bavarian Nordic/GSF”) and Bio Blue Bird entered into a non-exclusive License Agreement (“Bavarian Nordic/GSF License Agreement”) in July 2005, whereby Bio Blue Bird was granted a non-exclusive license to further develop, make, have made (including services under contract for Bio Blue Bird or a sub-licensee, by Contract Manufacturing Organizations, Contract Research Organizations, Consultants, Logistics Companies or others), obtain marketing approval, sell and offer for sale the clinical data generated from the pancreatic cancer clinical trials that used the cells and capsules developed by Bavarian Nordic/GSF (then known as “CapCells™”) or otherwise use the licensed patent rights related thereto in the countries in which patents had been granted. Bio Blue Bird was required to pay Bavarian Nordic a royalty of 3% of the net sales value of each licensed product sold by Bio Blue Bird and/or its Affiliates and/or its sub-licensees to a buyer. The term of the Bavarian Nordic/GSF License Agreement continued on a country-by-country basis until the expiration of the last valid claim of the licensed patent rights.
Bavarian Nordic/GSF and Bio Blue Bird amended the Bavarian Nordic License Agreement in December 2006 (“First Amendment to Bavarian Nordic/GSF License Agreement”) to reflect that: (i) the license granted was exclusive; (ii) a royalty rate increased from 3% to 4.5%; (iii) Bio Blue Bird assumed the patent prosecution expenses for the existing patents; and (iv) to make clear that the license will survive as a license granted by one of the licensors if the other licensor rejects performance under the Bavarian Nordic License Agreement due to any actions or declarations of insolvency.
In June 2013, we acquired from Austrianova an exclusive, worldwide license to use the Cell-in-a-Box® technology and trademark for the development of a therapy for Type 1 and insulin-dependent Type 2 diabetes (“Diabetes Licensing Agreement”). This allows us to develop a therapy to treat diabetes through encapsulation of a human cell line that has been genetically modified to produce, store and release insulin in response to the levels of blood sugar in the human body.
In October 2014, we entered into an exclusive, worldwide license agreement with the UTS (“Melligen Cell License Agreement”) in Australia to use insulin-producing genetically engineered human liver cells developed by UTS to treat Type 1 diabetes and insulin-dependent Type 2 diabetes. These cells, named “Melligen,” were tested by UTS in mice and shown to produce insulin in direct proportion to the amount of glucose in their surroundings. In those studies, when Melligen cells were transplanted into immunosuppressed diabetic mice, the blood glucose levels of the mice became normal. In other words, the Melligen cells reportedly reversed the diabetic condition.
| 16 |
In December 2014, we acquired from Austrianova an exclusive, worldwide license to use the Cell-in-a-Box® technology and trademark in combination with genetically modified non-stem cell lines which are designed to activate cannabinoid prodrug molecules for development of therapies for diseases and their related symptoms using of the Cell-in-a-Box® technology and trademark (“Cannabis Licensing Agreement”). This allows us to develop a therapy to treat cancer and other diseases and symptoms through encapsulation of genetically modified cells designed to convert cannabinoids to their active form using the Cell-in-a-Box® technology and trademark.
In July 2016, we entered into a Binding Memorandum of Understanding with Austrianova (“Austrianova MOU”). Pursuant to the Austrianova MOU, Austrianova will actively work with us to seek an investment partner or partners who will finance clinical trials and further develop products for our therapy for cancer, in exchange for which we, Austrianova and any future investment partner will each receive a portion of the net revenue from the sale of cancer products.
In October 2016, Bavarian Nordic/GSF and Bio Blue Bird further amended the Bavarian Nordic License Agreement (“Second Amendment to Bavarian Nordic/GSF License Agreement”) in order to: (i) include the right to import in the scope of the license; (ii) reflect ownership and notification of improvements; (iii) clarify which provisions survive expiration or termination of the Bavarian Nordic License Agreement; (iv) provide rights to Bio Blue Bird to the clinical data after the expiration of the licensed patent rights; and (v) change the notice address and recipients of Bio Blue Bird.
In May 2018, the Company entered into a series of binding term sheet amendments (“Binding Term Sheet Amendments”). The Binding Term Sheet Amendments provide that our obligation to make milestone payments to Austrianova is eliminated in their entirety under the: (i) Cannabis License Agreement; and (ii) the Diabetes License Agreement, as amended. The Binding Term Sheet Amendments also provide that our obligation to make milestone payments to SG Austria for therapies for cancer be eliminated in their entirety. In addition, the Binding Term Sheet Amendments also provides that the scope of the Diabetes License Agreement is expanded to include all cell types and cell lines of any kind or description now or later identified, including, but not limited to, primary cells, mortal cells, immortal cells and stem cells at all stages of differentiation and from any source specifically designed to produce insulin for the treatment of diabetes.
In addition, one of the Binding Term Sheet Amendments provides that we will have a 5-year right of first refusal from August 30, 2017 in the event that Austrianova chooses to sell, transfer or assign at any time during this period the Cell-in-a-Box® technology, tradename and Associated Technologies (defined below), intellectual property, trade secrets and know-how, which includes the right to purchase any manufacturing facility used for the Cell-in-a-Box® encapsulation process and a non-exclusive license to use the special cellulose sulfate utilized with the Cell-in-a-Box® encapsulation process (collectively, “Associated Technologies”); provided, however, that the Associated Technologies subject to the right of first refusal do not include Bac-in-a-Box® (which is used to encapsulate bacteria). Additionally, for a period of one year from August 30, 2017 one of the Binding Term Sheet Amendments provides that Austrianova will not solicit, negotiate or entertain any inquiry regarding the potential acquisition of the Cell-in-a-Box® and its Associated Technologies.
The Binding Term Sheet Amendments further provide that: (i) the royalty payments on gross sales as specified in the SG Austria APA, the Cannabis License Agreement and the Diabetes License Agreement are changed to 4%; and (ii) the royalty payments on amounts received by us from sublicensees on sublicensees’ gross sales under the same agreements are changed to 20% of the amount received us from our sublicensees, provided, however, that in the event the amounts received by us from sublicensees is 4% or less of sublicensees’ gross sales, Austrianova will receive 50% of what we receive (up to 2%) and then additionally 20% of any amount we receive over that 4%.
One of the Binding Term Sheet Amendments requires that we pay $900,000 to Austrianova ratably over a nine-month period in the amount of two $50,000 payments each month during the nine-month period on the days of the month to be agreed upon between the parties, with a cure period of 20 calendar days after receipt by us of written notice from Austrianova that we have failed to pay timely a monthly payment. As of April 30, 2020, the $900,000 amount has been paid in full. The Binding Term Sheet Amendments also provide that Austrianova receives 50% of any other financial and non-financial consideration received from our sublicensees of the Cell-in-a-Box® technology.
| 17 |
Goal and Strategies to Implement
Our goal is to become an industry-leading biotechnology company using the Cell-in-a-Box® technology as a platform upon which therapies for cancer, malignant ascites and diabetes are developed and obtain marketing approval for these therapies from regulatory agencies in the U.S., the European Union, Australia and Canada.
Our strategies to implement our goal consist of the following:
| · | Submission of our response to the FDA’s clinical hold and for the FDA to allow us to commence a clinical trial in LAPC; | |
| · | Completion of preclinical studies and clinical trials that demonstrate the effectiveness of our product candidate in reducing the production and accumulation of malignant ascites fluid in the abdomen that is characteristic of pancreatic and other abdominal cancers; | |
| · | Completion of preclinical studies and clinical trials that involve the encapsulation of the Melligen cells and genetically modified stem cells using the Cell-in-a-Box® technology to develop a therapy for Type 1 and insulin-dependent Type 2 diabetes; | |
| · | Acquisition of contracts that generate revenue or provide research and development capital utilizing our sublicensing rights; | |
| · | Further development of uses of the Cell-in-a-Box® technology platform through contracts, licensing agreements and joint ventures with other companies; and | |
| · | Completion of testing, expansion and marketing of existing and newly derived product candidates. |
Market Opportunity and Competitive Landscape
The three areas we are developing for live cell encapsulation-based therapies are cancer, diabetes and malignant ascites.
The Cell-in-a-Box® capsules are comprised of cotton’s natural component - cellulose. Other materials used by competitors include alginate, collagen, chitosan, gelatin and agarose. Alginate appears to be the most widely used of these. We believe the inherent strength and durability of our cellulose-based capsules provides us with advantages over the competition. They do so with no evidence of rupture, damage, degradation, fibrous overgrowth or immune system response. The cells within the capsules also remained alive and functioning during these studies. Other encapsulating materials degrade in the human body over time, leaving the encapsulated cells open to immune system attack. Damage to surrounding tissues has also been reported to occur over time when other types of encapsulation materials begin to degrade.
The cells encapsulated using the Cell-in-a-Box® technology can be frozen for extended periods of time. When thawed, the cells are recovered with approximately 85% viability. We are unaware of any other cell encapsulation material that is capable of protecting their encapsulated cells to this degree. The implications of this property of the Cell-in-a-Box® technology are obvious - long-term storage of encapsulated cells and shipment of encapsulated cells over long distances.
We believe our live cell encapsulation technology may have significant new advantages and opportunities for us in numerous and developing ways. For example:
| · | Cancerous diseases may be treated by placing encapsulated drug-converting cells that convert a chemotherapy prodrug near the cancerous tumor; | |
| · | Confinement and maintenance of therapeutic cells that activate a chemotherapy prodrug may be placed at the site of implantation in a blood vessel near the cancerous tumor results in “targeted chemotherapy”; | |
| · | Increased efficacy of a chemotherapy prodrug may allow for lower doses of the prodrug to be given to a patient, significantly reducing or even eliminating side effects from the chemotherapy; | |
| · | Encapsulating genetically modified live cells has the potential for the treatment of systemic diseases of various types, including diabetes; | |
| · | Multi-layered trade secret protection and marketing exclusivity for our technology exists and is being expanded; | |
| · | Cell-in-a-Box® capsules can prevent immune system attack of functional cells inside them without the need for immunosuppressive drug therapy; and | |
| · | Promising data with the Cell-in-a-Box® technology and the cells used with our technology from animal and initial human clinical trials. |
| 18 |
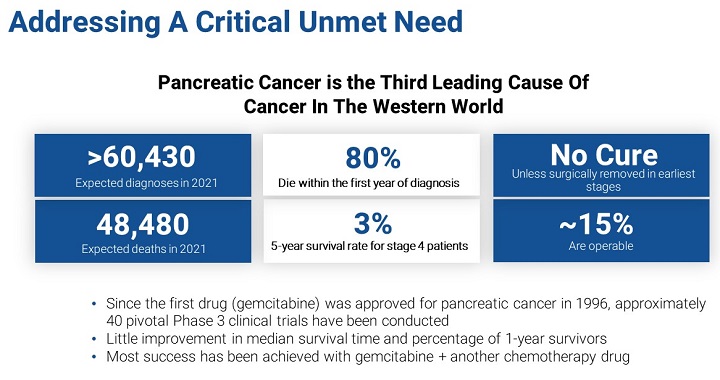
Pancreatic cancer is increasing in most industrialized countries. The American Cancer Society estimates that in 2022 there will be 62,210 people in the U.S. diagnosed with pancreatic cancer. It also estimates 48,830 patients with pancreatic cancer will die in 2022. Pancreatic cancer accounts for about 3% of all cancers in the U.S. and about 7% of all cancer deaths.
Our goal is to satisfy a clear unmet medical need for patients with LAPC whose tumors no longer respond after 4-6 months of treatment with the chemotherapy combination of Abraxane® plus gemcitabine or the four-drug combination known as FOLFIRINOX. For these patients, there is currently no effective therapy. We believe there will be no therapy comparable to our Cell-in-a-Box® plus low dose of ifosfamide combination therapy when it is used in these patients.
We face intense competition in the field of treating pancreatic cancer. There are dozens of startups, smaller biotech companies, big pharma, and several academic institutions and cancer centers all trying to improve the outcome for pancreatic cancer patients. For example, in a single patient case report published June 2022 in the New England Journal of Medicine, a study funded by the Providence Portland Medical Foundation in conjunction with the Earle A. Chiles Research Institute reported objective regression of metastatic pancreatic cancer using genetically-engineered autologous T cells. There are several drugs already available and in the pipelines of pharmaceutical companies worldwide, not the least of which is the combination of the drugs of Abraxane® and gemcitabine. This is the primary FDA-approved combination of drugs for treating advanced pancreatic cancer. In Europe and in the U.S., the 4-drug combination FOLFIRINOX has also found use as a first-line treatment for advanced pancreatic cancer. Some of our competitive strengths include the Orphan Drug Designation we have been granted by the FDA and the European Medicines Agency for our pancreatic cancer therapy, our trade secrets, the patents we are seeking and the licensing agreements we have that are described in this Report. Yet many of our competitors have substantially greater financial and marketing resources than we do. They also have stronger name recognition, better brand loyalty and long-standing relationships with customers and suppliers. Our future success will be dependent upon our ability to compete.
We believe our product candidate for pancreatic cancer has already shown promise through the completion of a Phase 1/2 and a Phase 2 clinical trial in advanced, inoperable pancreatic cancer carried out in Europe by Bavarian Nordic in 1998 – 1999 and 2000, respectively.
We have a number of competitors developing Cannabis-based treatments for cancer. In February 2021, Jazz Pharmaceuticals Public Limited Company (“Jazz”), a neuroscience and oncology focused company, acquired GW Pharmaceuticals, PLC for $7.2 billion. Jazz now has two approved cannabinoid extract-based products: Epidiolex® (CBD) oral solution for the treatment of seizures associated with Lennox-Gastaut syndrome, Dravet syndrome or tuberous sclerosis complex, and Sativex® (THC/CBD) oromucosal spray for the treatment of severe multiple sclerosis spasticity. Sativex® is currently being studied in conjunction with the Brain Tumour Charity and the UK National Health Service to examine effectiveness in the treatment of recurrent glioblastoma brain tumor when used alongside the chemotherapeutic agent temozolomide. Jazz’s pipeline indications include: neonatal hypoxic-ischemic encephalopathy, neuropsychiatry targets, autism spectrum disorders, epilepsy, spasticity and undisclosed targets. Cannabis Science, Inc. (“CBIS”) has a number of indications in its product development pipeline, all pre-clinical, the most advanced being for the treatment of oxidative stress, psychosis/anxiety, PTSD, and sleep deprivation. CBIS also has plans to develop treatments for Stage 4 lung cancer and pancreatic cancer. CNBX Pharmaceuticals Inc. (previously Cannabics Pharmaceuticals, Inc.) (“CNBX”) has a primary research focus on the development of cannabinoid therapies for the treatment of cancer, mainly cancers of the gastrointestinal tract, skin, breast and prostate. CNBX’s other Cannabis-based areas of research include Alzheimer’s disease, mental health conditions, and auto-immune diseases. Cannabotech Ltd. (“Cannabotech”), an Israeli company, in collaboration with Haifa University, is studying an improved method for killing pancreatic and colon cancer cells using a botanical drug based on an extract of the Cyathus striatus fungus and a cannabinoid extract. Cannabotech is also developing therapies for breast, lung and prostate cancers.
In contrast to the work being done by these companies, we plan to focus on developing specific therapies based on chosen molecules rather than using Cannabis extracts. We intend to use the Cell-in-a-Box® technology in combination with genetically -modified cell lines designed to activate cannabinoid molecules for the targeted treatment of diseases and their related symptoms.
The Centers for Disease Control and Prevention estimates that in 2022 a total of 37.3 million people in the U.S. have been diagnosed with diabetes (11.3% of the U.S. population) and another 8.5 million people (23.0% of adults) are undiagnosed. The diabetes market is estimated in the tens of billions of dollars, and it continues to grow.
| 19 |
The field of diabetes cell therapy development is very competitive. There are numerous companies developing cell-based therapies for diabetes. These competitors include companies such as ViaCyte, Inc. which has two stem cell-based product candidates in Phase 1/2 clinical trials for type 1 diabetes: PEC-Direct, which is a pouch that is “open” to the surrounding vasculature and requires the use of immunosuppressive drugs, and PEC-Encap, which is a pouch that contains the implanted cells and prevents contact with the vasculature and immune cells but still allows passage of nutrients and proteins to travel between the cells inside the device and blood vessels which grow along the outside of the device. PEC-Encap is reported to generally prevent immune rejection and immune sensitization. Conceptually, PEC-Encap has similarities with Cell-in-a-Box®. Other companies developing some form of encapsulation-based diabetes therapy include Vertex Pharmaceuticals Inc., Defymed, Diatranz Otsuka Limited, Seraxis, Inc., Unicyte AG, Sernova Corp., Betalin Therapeutics Ltd., Novo Nordisk, Beta-O2 Technologies Ltd., Eli Lilly & Co. in collaboration with Sigilon Therapeutics, Inc. and the Diabetes Research Institute Foundation.
Although such competition exists in the diabetes space, we believe these other companies are developing encapsulation-based therapies using materials and methodologies that produce capsules or devices that are far less robust than ours or that are associated with other problems, such as extremely short shelf-life of the product and/or fibrotic overgrowth of their encapsulation products when implanted in the body. We believe these properties are not characteristic of the Cell-in-a-Box® capsules. Our product candidate for diabetes has shown promise. Completed research studies have resulted in positive responses in animal models using the Melligen cells. We believe we are in a strong competitive position considering our unique encapsulation technology and the genetically modified cells that we have the exclusive worldwide license to use in most industrialized countries.
Malignant ascites occurs when cancer cells irritate the peritoneum causing an overproduction of ascitic fluid which causes the abdomen to swell as fluid accumulates. It is more likely to develop in patients who have ovarian, uterine, cervical, colorectal, stomach, pancreatic, breast and liver cancers. In most patients, development of malignant ascites is a sign of advanced disease and poor prognosis. Malignant ascites can result in impairment to the quality of life of a cancer patient. In addition to abdominal distention, pain and difficulty breathing, it may also cause nausea, vomiting, early satiety, lower extremity edema, weight gain and reduced mobility. These symptoms can interfere with a patient’s ability to eat, to walk and to perform daily activities. They also reduce a patient’s ability to withstand anti-cancer therapies, potentially reducing survival.
We are developing a therapy to delay the production and accumulation of malignant ascites using our cancer therapy (i.e., ifosfamide converting encapsulated live cells). Preclinical studies are underway in Germany, and, if successful, we plan to seek FDA approval to conduct a Phase 1 study. Typical treatments for malignant ascites include paracentesis, percutaneously implanted catheters, peritoneal ports and peritoneovenous shunts. These treatments can be painful, ineffective and expensive. There is currently no available treatment that delays the production and accumulation of malignant ascites fluid, and we know of no competitors in this area.
Previous Clinical Trials Using Encapsulation Technology
| 20 |
Two previous clinical trials using what is now our encapsulation technology were carried out in Europe by Bavarian Nordic in 1998-1999 and 2000, respectively. Both employed the combination of the cellulose-based live cell encapsulation technology with low doses of the anticancer drug ifosfamide. However, the FDA may not accept the results of these trials for various reasons, none of which are in our control. In such event, we may have to conduct a Phase 1 trial, not a Phase 2b trial, or even further pre-clinical animal trials.
The results of the two clinical trials have been published in the peer-reviewed scientific literature and are summarized as follows:
Phase 1/2 Clinical Trial
Dates of Trial and Location: This clinical trial was opened on July 28, 1998 and closed on September 20, 1999. It was carried out at the Division of Gastroenterology, University of Rostock, Germany.
Identity of Trial Sponsors: The clinical trial was sponsored by Bavarian Nordic.
Trial Design: The clinical trial was an open-label, prospective, single-arm and single center trial.
Patient Information: A total of 17 patients were enrolled in the clinical trial (51 were screened). A total of 14 patients were treated because two of the original 17 patients developed severe infections before the start of the clinical trial and had to be treated by other means. For the other patient, angiography was not successful, causing the patient to be disqualified from participating in the clinical trial.
Trial Criteria: Criteria for enrolling in the clinical trial included inoperable pancreatic adenocarcinoma Stage 3-4 (according to IUCC criteria) as determined by histology and measured by computerized tomography (“CT”) scan and the patients must not have had any prior chemotherapy for their disease.
Duration of Treatment and Dosage Information: On day 0, celiac angiography was performed and 300 (in 13 patients, 250 in one) of the capsules containing the ifosfamide-activating cells were placed by supraselective catheterization of an artery leading to the tumor. Each capsule (~0.7 mm in diameter) contained about 20,000 cells. The cells overexpressed CYP2B1 (a cytochrome P450 isoform), which catalyzed the conversion of the anticancer prodrug ifosfamide into its “cancer-killing” form.
On day 1, patients were monitored for evidence of any clinically relevant adverse reactions, e.g., allergy and/or pancreatitis. On days 2-4, each patient received low-dose (1 g/m2 body surface area) ifosfamide in 250 ml of normal saline administered systemically as a 1-hour infusion. This was accompanied by a 60% dose equivalent of the uroprotective drug Mesna, which is used to reduce the side effects of ifosfamide chemotherapy, given as three intravenous injections. This regimen was repeated on days 23-25 for all but two patients who received only one round of ifosfamide. A total of only two cycles of ifosfamide were given to the remainder of the patients.
Specific Clinical Endpoints: Median survival time from the time of diagnosis, the percentage of patients who survived one year or more and the quality of life of each patient were examined in the clinical trial.
Observational Metrics Utilized and Actual Results Observed: Standard National Cancer Institute (“NCI”) criteria for evaluating tumor growth were used to assess results:
| · | stable disease (tumors 50-125% of initial size) (“SD”); | |
| · | partial remission (more than 50% reduction in tumor volume) (“PR”); and | |
| · | minor response (tumor reduction of between 25% and 50%) (“MR”). |
Effects of the treatment on tumor size were measured by CT scans. Control CT scans were scheduled for weeks 10 and 20, respectively. During the final visit, a control angiography was performed. On the initial CT scan, the scan demonstrating the largest diameter of the primary tumor was identified and the area measured. Using appropriate landmarks, an identical scan was used for comparison. CT scans were evaluated by two unrelated radiologists, one of whom was not involved in the clinical trial. After formally finishing the clinical trial, patients were followed on an ambulatory basis with visits once every three months.
| 21 |
Toxicity was measured based on World Health Organization (“WHO”)/NCI guidelines on common toxicity criteria. The WHO and the NCI use standardized classifications of the adverse events associated with the use of cancer drugs. In cancer clinical trials, these are used to determine if a drug or treatment causes unwanted side effects (“Adverse Events”) when used under specific conditions. For example, the most commonly used classification is known as the “Common Terminology Criteria for Adverse Events” developed by the NCI in the U.S. Most clinical trials carried out in the U.S. and the United Kingdom code their Adverse Event. This system consists of five grades. These are: 1 = mild; 2 = moderate; 3 = severe; 4 = life-threatening; 5 = death. In the studies reported for Cell-in-a-Box® plus low-dose ifosfamide combination in pancreatic cancer patients, the study investigators noted 11 Serious Adverse Events (“SAEs”) in 7 patients, none of which were believed to be treatment-related.
Each patient’s need for pain medication and the quality of life (“QOL”) was monitored using a questionnaire established for diseases of the pancreas. A QOL questionnaire for cancer patients, QLQ-C30, had been validated in several languages, but the module for pancreatic cancer per se was still under development at the time of the study with respect to reliability, sensibility against changes and multicultural validation. Accordingly, a version of the core questionnaire and a German QOL scale (published in 1995) for pancreatic cancer patients was used. QOL data were documented independently from safety and efficacy data by having patients complete an independent questionnaire. Assessment of QOL data did not interfere with routine documentation of Adverse Events reported by the patients. QOL questionnaires were analyzed according to the criteria developed by the European Organization for Research and Treatment of Cancer (“EORTC”). As used in the description of the QOL results discussed in the published report of the Phase 1/2 trial of the Cell-in-a-Box® plus low-dose ifosfamide combination in pancreatic cancer patients, the questionnaire was used to assess the QOL of patients undergoing treatment. The QOL was analyzed in a similar manner to the way that a QOL questionnaire developed by the EORTC is usually analyzed. This latter questionnaire is known as EORTC QLQ-C30. QOL data were available from the baseline evaluation for 14 patients and for analysis of change for 8 patients.
A clinical benefit score based on variables, including the “Karnofsky Score” and body weight, was determined. Pain and analgesic consumption were calculated from the QOL questionnaires. The Karnofsky Score is a scale that is used to attempt to quantify a cancer patient’s general well-being and activities of daily life. It is often used to judge the suitability of patients for inclusion into clinical trials. As a clinical trial progresses, a patient’s Karnofsky Score can change. It is also used to assess a patient’s QOL as a clinical trial progresses. The scale starts at 100 (normal, no complaints, no evidence of disease) and decreases in decrements of 10 down through 50 (requires considerable assistance and frequent medical care) all the way to 10 (moribund, fatal processes progressing rapidly) and finally to 0 (deceased). Pain intensity was measured on a visual analog scale ranging from 0 (no pain) to 100 (the most intensive pain imaginable) in increments of 10. Analgesic consumption was assessed using a separate scale in which 0 indicated no regular consumption of analgesics and 25, 50 and 100 indicated administration of non-steroidal anti-inflammatory drugs or opiates several times per year, per month or per week, respectively.
The primary tumor did not grow in any of the 14 patients. Two patients had a PR; 12 patients exhibited SD; and two patients showed an MR.
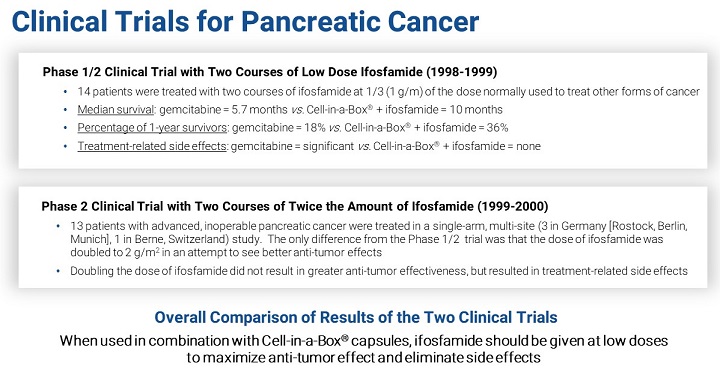
Median survival time of patients in this clinical trial was 39 weeks. The one-year survival rate was 36%.
Within the 20-week study period, three patients died from disease progression (on days 9, 85 and 132). Upon postmortem examination, the patient who died on day 9 from recurrent pulmonary embolism was found to have extensive tumor necrosis.
The chemotherapy regimen was well tolerated. No toxicity beyond Grade 2 (moderate adverse effect) was detected in any of the 14 patients.
Eleven SAEs were seen in 7 patients during the study period. None of them were treatment-related (due to capsule implantation or ifosfamide administration). These SAEs were attributed to underlying disease and/or the effects associated with the disease.
Implanting the capsules did not result in any obvious allergic or inflammatory response, and no patients developed pancreatitis during the trial. Some patients exhibited elevated amylase levels, presumably due to tumor infiltration of the pancreas and limited obstructive chronic pancreatitis. However, no further increase in amylase levels was seen after angiography and capsule implantation.
In accordance with the report of the study, only one Adverse Event (increased lipase activity on day 15 after installation of the capsules), which was a Grade 1 Adverse Event, “may” have been linked to implanting the capsules.
| 22 |
Ten of 14 patients experienced a “clinical benefit” which means either no increase or a decrease in pain intensity. For 7 of the patients, this was confirmed by their analgesic consumption. None of these “benefited” patients registered an increased analgesic usage either in terms of dosage or WHO levels.
None of the patients showed an increased Karnofsky Score after treatment. However, 7 of the 14 patients had stable Karnofsky Scores at the week 10 assessment. For 4 of these patients, their indices were still stable at the week 20 assessment.
One patient’s body weight increased at both weeks 10 and 20 and another patient showed increased weight at week 10 (this patient withdrew from the clinical trial and no week 20 weight was obtained). Two patients showed stable body weights at week 10, one of whom dropped out of the clinical trial and the other showed weight loss at week 20.
Two scenarios were used to establish the overall integrative clinical benefit response, where each patient was given a +2 score for an improved value, a +1 score for a stable value and a -1 score for a worsened value for each of four criteria (pain, analgesic consumption, Karnofsky Score and body weight) as compared to the relevant week 0 values.
The “worst case scenario” required a pain relief score of 20 points or more to be judged an improvement and a decrease in the Karnofsky Score of 10 points or more to indicate worsening. Using this scenario, 50% or 7 of the treated patients experienced clinical benefit; 21.4% or 3 patients were neutral (benefits were offset by impairments); and 28.6% or 4 patients had no clinical benefit. The latter included those passing away before the median survival time.
In the “best case scenario,” a pain relief score of 10 points or more was an improvement. A decrease in Karnofsky Score of 20 points or more was considered a worsening. In this scenario, 71.4% or 10 patients had clinical benefit, 14.2% of patients showed neither benefit nor deterioration and 14.3% patients had no benefit.
Standard of Care: At the time this clinical trial was conducted, only one FDA-approved treatment for advanced, inoperable pancreatic cancer was available. That was the drug gemcitabine, first approved by the FDA in 1996.
An examination of the prescribing information for gemcitabine reflects that the median survival seen in the Phase 3 pancreatic cancer clinical trial for gemcitabine was approximately 23 weeks (5.7 months). The percentage of one-year survivors was approximately 18%. In a Phase 3 clinical trial of Celgene’s Abraxane® plus gemcitabine combination that was approved by the FDA in September 2013, the median survival time for patients was about 8.5 months and the percentage of one-year survivors was approximately 35%.
The treatment with gemcitabine of patients with pancreatic cancer is often associated with severe side effects. According to the prescribing information for gemcitabine, for use to treat pancreatic cancer the recommended dose is 1000 mg/m2 given intravenously over 30 minutes. The schedule of administration is weeks 1-8, weekly dosing for 7 weeks followed by one-week rest and then after week 8, weekly dosing on days 1, 8 and 15 of 28-day cycles.
Reductions in the doses of gemcitabine are necessitated by the occurrence of myelosuppression. Permanent discontinuation of gemcitabine is necessary for any of the following:
| · | unexplained dyspnea or other evidence of severe pulmonary toxicity; | |
| · | severe hepatotoxicity; | |
| · | hemolytic-uremic syndrome; | |
| · | capillary leak syndrome; and | |
| · | posterior reversible encephalopathy syndrome. |
Gemcitabine should be withheld, or its dose reduced by 50% for other severe (Grade 3 or 4) non-hematologic toxicity until that toxicity is resolved.
Conclusions: In the opinion of the trial’s investigators, in this Phase 1/2 clinical trial the use of the combination of Cell-in-a-Box® capsules plus low-dose ifosfamide was both safe and effective. This assessment was not based on the opinion of any drug regulatory authority and does not guarantee that that this assessment will be maintained in any late-phase clinical trial or that any drug regulatory authority will ultimately determine that the Cell-in-a-Box® plus low-dose ifosfamide combination is safe and effective for the purposes of granting marketing approval.
| 23 |
In the Phase 1/2 clinical trial only a small number of patients were evaluated. Statistical parameters were not used in the published reports of the Phase 1/2 trial to validate the anticancer efficacy of the Cell-in-a-Box® plus low-dose ifosfamide combination in patients with advanced, inoperable pancreatic cancer. In the opinion of the investigators, the results indicate a trend towards efficacy; accordingly, the results should not be viewed as absolute numbers. It should be noted, however, that because the results were not statistically significant, any observations of efficacy must be weighed against the possibility that the results were due to chance alone. The purpose of the clinical trial was not to obtain data so that marketing approval could be obtained from regulatory authorities. Rather, the clinical trial allowed the investigators to determine whether the Cell-in-a- Box® capsules plus low-dose ifosfamide combination holds promise as a therapy for advanced pancreatic cancer. In the cancer arena, Phase 1/2 clinical trials are intended to: (i) establish the safety of the drug or treatment being investigated; and (ii) determine if a trend towards efficacy exists. In accordance with FDA regulations and guidance, as well as similar regulations and guidance from other regulatory authorities in countries other than the U.S., we realize that a large, multicenter, randomized, comparative study needs to be conducted and the results from such a trial would have to confirm the results from this previous Phase 1/2 trial before an application for marketing approval could be filed with the FDA or EMA.
If our product candidate is approved by the regulatory agencies, we believe it could provide a significant benefit to those with this devastating and deadly disease, not only in terms of lifespan but also in terms of increased quality of life. Also, we believe that success of the live cell encapsulation technology in the pancreatic cancer setting may lead to its successful use in developing therapies for other forms of solid cancerous tumors after preclinical studies and clinical trials have been completed.
Phase 2 Clinical Trial
Location of Trial: The clinical trial was opened on November 16, 1999 and closed on December 1, 2000. This clinical trial was carried out at four centers in two countries in Europe. These were in Berne, Switzerland, and in Rostock, Munich and Berlin, Germany.
Trial Sponsor: The clinical trial was sponsored by Bavarian Nordic.
Trial Design: This was an open-label, prospective, single-arm multi-site study.
Patient Information: All 13 patients enrolled in the trial were treated. Twelve patients exhibited Stage 4 disease. The remaining patient had Stage 3 disease. Ten of the 13 patients exhibited metastases.
Duration of Treatment and Dosage Information: The number of capsules implanted varied from 221 to 300 with a mean of 244. On day 1, patients were monitored for any allergic reactions to capsule implantation and/or pancreatitis. The administration schedule of the treatment was the same as in the earlier Phase 1/2 trial, except that in this Phase 2 trial the dose of ifosfamide was doubled to 2 g/m2. In the Phase1/2 trial, it was 1g/m2. On days 2-4, patients received 2 g/m2 in normal saline as a one-hour infusion. The urinary tract protector Mesna was also given as 3 intravenous injections. This regimen was repeated on days 23-25.
Specific Clinical Endpoints: The primary endpoint of the trial was to determine response rate as defined by SD, PR and MR as well as the clinical benefit (Karnofsky score) of the treatment. The timing of the tumor size measurements and determination of tumor sizes by CT scans were done by independent radiologists. A secondary endpoint was to determine time to progression, tumor response, duration of partial or complete remission, length of symptom-free survival, survival time and quality of life. Another secondary endpoint was to evaluate the safety and tolerability of the treatment regimen, with attention being paid to the appearance of pancreatitis or immediate allergic reactions.
Safety Analysis of Angiography, Capsule Implantation and Chemotherapy: On average, angiography took approximately 40 minutes. For 5 of the patients in this clinical trial, more than one blood vessel had to be used for placement of the capsules. The administration of the capsules was well tolerated. There were no signs of allergic reactions or hemorrhagic cystitis after implantation of the capsules. Two patients had increased levels of serum lipase at baseline. After additional measurements, these were not considered to be clinically relevant. The dose of ifosfamide (2 g/m2) used was found to be toxic in most patients. This resulted in one patient having to reduce the ifosfamide dose in the second of the two cycles of treatment with the drug. The most common toxic effects were nausea, vomiting, malaise, anorexia and mild hematuria.
| 24 |
Serious Adverse Events: A total of 16 SAEs were documented in eight patients, including 3 SAEs leading to death. None of these SAEs were attributed to placement of the encapsulated cells. One patient experienced neurological impairment (drowsiness, nocturnal enuresis, mild somnolence) which was attributed to treatment with the 2 g/m2 dose of ifosfamide. All patients experienced between 5 and 19 SAEs. Six SAEs were rated as life-threatening; 10.2% were rated as severe; 28.7% were rated as moderate; and 53.7% were rated as mild. None of the SAEs was thought to be related to placement of the encapsulated cells, but 44% were related to the administration of ifosfamide at the elevated dose given. Most frequent SAEs were alopecia, anemia, leucopenia, nausea and vomiting or encephalopathy. Other SAEs were new or worse symptoms of the patients’ underlying disease. A total of 65 events met the NCI’s common toxicity criteria. Of these, 46.2% had Grade 1, 40% had Grade 2, 9.2% had Grade 3 and 4.6% had Grade 4 toxicities.
Tumor Reductions and Patient Survival Results: The size of the primary tumor was measured before starting the live cell encapsulation plus ifosfamide therapy and at weeks 10 and 20 post-treatment. No PRs were observed, but 4 patients exhibited tumor size reductions, 4 patients showed tumor growth and the remaining 5 patients had SD over the “follow-up” period after chemotherapy.
The median survival of patients was 40 weeks. Most the survival benefit was shown early during the entire observation period. However, as time progressed, these patients succumbed at the same rate as historical controls. This observation suggested to the investigators that prolongation of the survival benefit might be achieved if additional courses of ifosfamide chemotherapy were given. The one-year survival rate was 23%. It was thought that this may be attributable to the higher dose of ifosfamide used in this clinical trial.
Quality of Life: An assessment of the quality of life of the patients was performed in this clinical trial. Quality of life data were available for all the patients. According to this QOL assessment, although pain during the night decreased, patients felt themselves to be less attractive and lost interest in sex. No additional improvements in patients’ quality of life were observed.
Conclusions: The opinions of the investigators were as follows: (i) the lack of “problems” associated with the implanted encapsulated cells was noted as in the Phase 1/2 trial; (ii) administering more than two courses of treatment with ifosfamide might have beneficial effects on survival; and (iii) since doubling the dose of ifosfamide from that used in the Phase 1/2 trial had no beneficial antitumor or survival effect but was associated with increased side effects from the treatment, the dose of ifosfamide to be used in combination with the encapsulated cells for all future trials should be 1 g/m2.
Manufacturing
We are outsourcing all cell growth, processing and encapsulation services needed for our future proposed clinical trials of the encapsulated cell-based cancer and diabetes product candidates. The Cell-in-a-Box® encapsulation will be done by Austrianova at its cGMP-compliant manufacturing facility in Bangkok, Thailand. The encapsulation process is proprietary to Austrianova. Austrianova is experiencing significant supply chain disruptions. We believe it may also be experiencing liquidity issues. If Austrianova is unwilling or unable to perform such manufacturing for us, we are not aware of any replacement manufacturer for the Cell-in-a-Box® technology.
In March 2014, we entered a Manufacturing Framework Agreement with Austrianova (“Manufacturing Framework Agreement”) pursuant to which Austrianova will encapsulate the genetically -engineered live cells that will be used for our product candidate for the treatment of cancer. We have also contracted with Austrianova to provide encapsulated insulin-producing cells for our preclinical studies in diabetes. At the appropriate time, we intend to enter into a similar manufacturing framework agreement with Austrianova for the encapsulated cells we will need for our product candidate for the treatment of diabetes.
Government Regulation and Product Approval
As a development -stage biotechnology company that operates in the U.S., we are subject to extensive regulation by the FDA and other federal, state, and local regulatory agencies. The federal Food, Drug, and Cosmetic Act (“FDCA”) and its implementing regulations set forth, among other things, requirements for the research, testing, development, manufacture, quality control, safety, effectiveness, approval, labeling, storage, record keeping, reporting, distribution, import, export, advertising, promotion, marketing and sale of our product candidates. Although the discussion below focuses on regulation in the U.S., we anticipate seeking approval for, and marketing of, our product candidates in other countries. Our activities in other countries will also be the subject of extensive regulation, although there can be important differences with the U.S. The process of obtaining regulatory marketing approvals and the subsequent compliance with appropriate federal, state, local and foreign statutes and regulations will require the expenditure of substantial time and financial resources and may not be successful.
| 25 |
Regulatory approval, when obtained, may be limited in scope which may significantly limit the uses for which a product may be placed into the market. Further, approved drugs or biologic products, as well as their manufacturers, are subject to ongoing post-marketing review, inspection and discovery of previously unknown issues regarding the safety and efficacy of such products or the manufacturing or quality control procedures used in their production. These may result in restrictions on their manufacture, sale or use or in their withdrawal from the market. Any failure or delay by us, our suppliers of manufactured drug product, collaborators or licensees in obtaining regulatory approvals could adversely affect the marketing of our product candidates and our ability to receive product revenue, license revenue or profit-sharing payments. For more information, see Item 1A. “Risk Factors.”
U.S. Government Regulation
The FDA is the main regulatory body that controls pharmaceuticals and biologics in the U.S. Its regulatory authority is based in the FDCA and the Public Health Service Act. Pharmaceutical products and biologics are also subject to other federal, state and local statutes and regulations. A failure to comply with any requirements during the product development, approval, or post-approval periods, may lead to administrative or judicial sanctions. These sanctions could include the imposition by the FDA or by an Institutional Review Board (“IRB”) of a hold on clinical trials, refusal to approve pending marketing applications or supplements, withdrawal of approval, warning letters, product recalls, product seizures, total or partial suspension of production or distribution, injunctions, fines, civil penalties or criminal prosecution.
The steps required before a new drug or biologic may be marketed in the U.S. generally include:
| · | completion of preclinical studies and formulation studies in compliance with the FDA’s Good Laboratory Practices (“GLP”), protocols and regulations; | |
| · | satisfactory completion of an FDA inspection of the manufacturing facilities at which the investigational product candidate is produced to assess compliance with cGMP and proof that the facilities, methods and controls are adequate; | |
| · | submission to the FDA of an IND to support human clinical testing in the U.S.; | |
| · | approval by an IRB at each clinical site before a trial may be initiated at that site; | |
| · | performance of adequate and well-controlled clinical trials in accordance with federal regulations and with Good Clinical Practices (“GCP”) to establish the safety and efficacy of the investigational product candidate for each target indication; | |
| · | Submission to the FDA of a New Drug Application (“NDA”) or a drug or Biologics License Application (“BLA”) for a biologic such as the therapies we are developing; | |
| · | satisfactory completion of an FDA Advisory Committee review, if applicable; and | |
| · | FDA review and approval of the NDA or BLA. |
Clinical Development
Before a drug or biologic product may be given to humans, it must undergo preclinical testing. Preclinical tests include laboratory evaluation of a product candidate’s chemical and biological activities and animal studies to assess potential safety and efficacy in humans. The results of these studies must be submitted to the FDA as part of an IND which must be reviewed by the FDA for safety and other considerations before testing can begin in humans.
An IND is a request for authorization from the FDA to administer an investigational product candidate to humans. This authorization is required before interstate shipping and administration can commence of any new drug or biologic product destined for use in humans in the U.S. A 30-day waiting period after the submission of each IND is required before commencement of clinical testing in humans. If the FDA has neither commented on nor questioned the IND within this 30-day period after submission of the IND, the clinical trial proposed in the IND may begin. A clinical trial involves the administration of the investigational product candidate to patients under the supervision of qualified investigators following GCP standards. These international standards are meant to protect the rights and health of patients and to define the roles of clinical trial sponsors, administrators and monitors. A clinical trial is conducted under protocols that detail the parameters to be used in monitoring safety, and the efficacy criteria to be evaluated. Each protocol involving testing on U.S. patients and subsequent protocol amendments must be submitted to the FDA as part of the IND.
| 26 |
The product candidates in our pipeline are at various stages of preclinical development. The path to regulatory approval includes three phases of clinical trials in which we collect data to support an application to regulatory agencies to allow us to ultimately market a product for treatment of a specified disease. There are many difficulties and uncertainties inherent in research and development of new products, and these can conceivably result in a high rate of failure. To bring a drug or biologic from the discovery phase to regulatory approval, and ultimately to market, takes years and the costs to do so are significant. Failure can occur at any point in the process, including after the product is approved, based on post-marketing factors. New product candidates that appear promising in development may fail to reach the market or may have only limited commercial success because of efficacy or safety concerns, inability to obtain necessary regulatory approvals, limited scope of approved uses, reimbursement challenges, difficulty or excessive costs of manufacture, alternative therapies or infringement of the patents or intellectual property rights of others. Uncertainties in the approval process of the regulatory agencies can result in delays in product launches and lost market opportunities. Consequently, it is exceedingly difficult to predict which products will ultimately be submitted for approval, which have the highest likelihood of obtaining approval and which will be commercially viable and generate profits. Successful results in preclinical or clinical studies may not be an accurate predictor of the ultimate safety or effectiveness of a product candidate.
Phase 1 Clinical Trial: A Phase 1 clinical trial begins when a regulatory agency, such as the FDA, allows initiation of the clinical investigation of a new product candidate. The clinical trial studies a product candidate’s safety profile and may include a preliminary determination of a product candidate’s safe dosage range. The Phase 1 clinical trial can also determine how a drug is absorbed, distributed, metabolized and excreted by the body and, therefore, the potential duration of its action.
Phase 2 Clinical Trial: A Phase 2 clinical trial is conducted on a limited number of patients; these patients can have a specific targeted disease. An initial evaluation of the product candidate’s effectiveness on patients is performed. Additional information on the product candidate’s safety and dosage range is obtained. For many diseases, a Phase 2 clinical trial can include up to several hundred patients.
Phase 3 Clinical Trial: A Phase 3 clinical trial is typically rigorously controlled, conducted in multiple centers and involves a larger target patient population that can consist of from several hundred to thousands of patients (depending on the disease being studied) to ensure that study results are statistically significant. During a Phase 3 clinical trial, physicians monitor patients to determine efficacy and to gather further information on safety. A Phase 3 clinical trial is designed to generate all the clinical data necessary to apply for marketing approval to a regulatory agency.
The decision to terminate development of an investigational product candidate may be made by either a health authority body, such as the FDA, by IRB/ethics committees, or by the sponsor for various reasons. The FDA may order the temporary or permanent discontinuation of a clinical trial at any time, or impose other sanctions, if it believes that the clinical trial either is not being conducted in accordance with FDA requirements or presents an unacceptable risk to the patients enrolled in the trial. In some cases, a clinical trial is overseen by an independent group of qualified experts organized by the trial sponsor, or the clinical monitoring board. This group provides authorization for whether a trial may move forward at designated checkpoints. These decisions are based on the limited access to data from the ongoing trial. The suspension or termination of development can occur during any phase of a clinical trial if it is determined that the patients are being exposed to an unacceptable health risk. There are also requirements for the registration of an ongoing clinical trial of a product candidate on public registries and the disclosure of certain information pertaining to the trial, as well as clinical trial results after completion.
A sponsor may be able to request a special protocol assessment (“SPA”), the purpose of which is to reach agreement with the FDA on the Phase 3 clinical trial protocol design and analysis that will form the primary basis of an efficacy claim. A sponsor meeting the regulatory criteria may make a specific request for a SPA and provide information regarding the design and size of the proposed clinical trial. A SPA request must be made before the proposed trial begins. All open issues must be resolved before the trial begins. If a written agreement is reached, it will be documented and made part of the record. The agreement will be binding on the FDA and may not be changed by the sponsor or the FDA after the trial begins, except with the written agreement of the sponsor and the FDA or if the FDA determines that a substantial scientific issue essential to determining the safety or efficacy of the product candidate was identified after the testing began. A SPA is not binding if new circumstances arise, and there is no guarantee that a study will ultimately be adequate to support an approval even if the study is subject to a SPA. Having a SPA does not guarantee that a product candidate will receive FDA approval.
Assuming successful completion of all required testing in accordance with all applicable regulatory requirements, detailed investigational product candidate information is submitted to the FDA in the form of an NDA or BLA to request regulatory approval for the product in the specified indication.
| 27 |
New Drug Applications and Biologic Licensing Applications
To obtain approval to market a drug or biologic in the U.S., a marketing application must be submitted to the FDA that provides data establishing the safety and effectiveness of the product candidate for the proposed indication. The application includes all relevant data available from pertinent preclinical studies and clinical trials, including negative or ambiguous results as well as positive findings, together with detailed information relating to the product’s chemistry, manufacturing and controls, as well as the proposed labeling for the product, among other things. Data can come from company-sponsored clinical trials intended to test the safety and effectiveness of a product, or from several alternative sources, including studies initiated by investigators. To support marketing approval, the data submitted must be sufficient in quality and quantity to establish the safety and effectiveness of the investigational product candidate to the satisfaction of the FDA.
In most cases, the NDA, in the case of a drug, or BLA, in the case of a biologic, must be accompanied by a substantial user fee. There may be some instances in which the user fee is waived. The FDA will initially review the NDA or BLA for completeness before it accepts the application for filing. The FDA has 60 days from its receipt of an NDA or BLA to determine whether the application will be accepted for filing based on the agency’s threshold determination that it is sufficiently complete to permit substantive review. After the NDA or BLA submission is accepted for filing, the FDA begins an in-depth review. The FDA has agreed to certain performance goals in the review of NDAs and BLAs. During a normal review cycle, a product is given an FDA action or Prescription Drug User Fee Act (“PDUFA”) date within 12 months of the submission if the submission is accepted. The FDA can extend this review by three months to consider certain late-submitted information or information intended to clarify information already provided in the submission. The FDA reviews the NDA or BLA to determine, among other things, whether the proposed product is safe and effective for its intended use, and whether the product is being manufactured in accordance with cGMP standards. The FDA may refer applications for novel product candidates which present difficult questions of safety or efficacy to an advisory committee. This is typically a panel that includes clinicians and other experts for review, evaluation and a recommendation as to whether the application should be approved and under what conditions. The FDA is not bound by the recommendations of an advisory committee, but it considers such recommendations carefully when making decisions.
Before approving an NDA or a BLA, the FDA will inspect the facilities at which the product is manufactured. The FDA will not approve the product candidate unless it determines that the manufacturing processes and facilities follow cGMP requirements and are adequate to assure consistent production of the product within required specifications. Manufacturers of human cellular or tissue-based biologics also must comply with the FDA’s Good Tissue Practices (“GTP”), as applicable, and with the general biological product standards. After the FDA evaluates the NDA or BLA and the sponsor company’s manufacturing facilities, it issues either an approval letter or a complete response letter. A complete response letter generally outlines the deficiencies in the submission and may require substantial additional testing or information for the FDA to reconsider the application. If, or when, those deficiencies have been addressed to the FDA’s satisfaction in a resubmission of the NDA or BLA, the FDA will issue an approval letter. Notwithstanding the submission of any requested additional information, the FDA ultimately may decide that the application does not satisfy the regulatory criteria for approval.
The time to final marketing approval can vary from months to years, depending on several variables. These variables can include such things as the disease type, the strength and complexity of the data presented, the novelty of the target or compound, risk-management approval and whether multiple rounds of review are required for the agency to evaluate the submission. After evaluating the NDA or BLA and all related information, including the advisory committee recommendation, if any, and inspection reports regarding the manufacturing facilities and clinical trial sites, the FDA may issue an approval letter, or, in some cases, a complete response letter. A complete response letter generally contains a statement of specific conditions that must be met in order to secure final approval of the NDA or BLA and may require additional clinical or preclinical testing in order for FDA to reconsider the application. Even with submission of this additional information, the FDA ultimately may decide that the application does not satisfy the regulatory criteria for approval. If and when those conditions have been met to the FDA’s satisfaction, the FDA will typically issue an approval letter. An approval letter authorizes commercial marketing of the drug or biologic with specific prescribing information, which may include contraindications, warnings or precautions, for certain indications. After approval, some types of changes to the approved product, such as adding new indications and additional labeling claims, are subject to further testing requirements and FDA review and approval.
| 28 |
Post Approval Regulations
After regulatory approval of a drug or biologic is obtained, a company is required to comply with certain post-approval requirements. For example, as a condition of approval of an NDA or BLA, the FDA may require post-marketing testing, including a Phase 4 clinical trial and surveillance to further assess and monitor the product’s safety and effectiveness after commercialization has begun. Also, as a holder of an approved NDA or BLA, a company is required to: (i) report adverse reactions and production problems to the FDA; (ii) provide updated safety and efficacy information; and (iii) comply with requirements concerning advertising and promotional labeling for any of its products. Also, quality control and manufacturing procedures must continue to conform to cGMP standards after approval to assure and preserve the long-term stability of the drug or biological product. The FDA periodically inspects manufacturing facilities to assess compliance with cGMP standards, which imposes extensive procedural and substantive record keeping requirements. Also, changes to the manufacturing process are strictly regulated, and, depending on the significance of the change, may require prior FDA approval before being implemented. In addition, FDA regulations require investigation and correction of any deviations from cGMP standards and impose reporting and documentation requirements upon a company and any third-party manufacturers that a company may decide to use. Manufacturers must continue to expend time, money and effort in production and quality control to maintain compliance with cGMP standards and other aspects of regulatory compliance.
Disclosure of Clinical Trial Information
A sponsor of a clinical trial of certain FDA-regulated products, including prescription drugs and biologics, is required to register and disclose certain clinical trial information on a public website. Information related to the product, patient population, phase of investigation, study sites and investigator involved, and other aspects of the clinical trial are made public as part of the registration. A sponsor is also obligated to disclose the results of a clinical trial after completion. Disclosure of the results can be delayed until the product or new indication being studied has been approved. Competitors may use this publicly available information to gain knowledge regarding the design and progress of our development programs.
Advertising and Promotion
The FDA and other federal regulatory agencies tightly regulate the marketing and promotion of drugs and biologics through, among other things, standards and regulations for direct-to-consumer advertising, communications regarding unapproved uses, industry-sponsored scientific and educational activities and promotional activities involving the internet. A product cannot be commercially promoted before it is approved. After approval, product promotion can include only those claims relating to safety and effectiveness that are consistent with the labeling approved by the FDA. Healthcare providers are permitted to prescribe drugs or biologics for “off-label” uses (uses not approved by the FDA and therefore not described in the drug’s labeling) because the FDA does not regulate the practice of medicine. However, FDA regulations impose stringent restrictions on manufacturers’ communications regarding off label uses. Broadly speaking, a manufacturer may not promote a product for off-label use, but may engage in non-promotional, balanced communication regarding off-label use under specified conditions. Failure to comply with applicable FDA requirements and restrictions in this area may subject a company to adverse publicity and enforcement action by the FDA, the U.S. Department of Justice (“DOJ”), the Office of the Inspector General of Health & Human Services (“HHS”) and state authorities. This could subject a company to a range of penalties that could have a significant commercial impact, including civil and criminal fines and/or agreements that materially restrict the manner in which a company promotes or distributes drug and biologics.
U.S. Patent Extension and Marketing Exclusivity
The Biologics Price Competition and Innovation Act (“BPCIA”) amended the PHSA to authorize the FDA to approve similar versions of innovative biologics, commonly known as biosimilars. A competitor seeking approval of a biosimilar must file an application to establish its product as highly like an approved innovator biologic, among other requirements. The BPCIA bars the FDA from approving biosimilar applications for 12 years after an innovator biological product receives initial marketing approval.
| 29 |
Depending upon the timing, duration and specifics of the FDA approval of the use of our product candidates, some of our U.S. patents, if granted, may be eligible for limited patent term extension under the Drug Price Competition and Patent Term Restoration Act of 1984 (“Hatch-Waxman Act”). The Hatch-Waxman Act permits a patent extension term of up to five years, as compensation for patent term lost during product development and the FDA regulatory review process. However, patent term extension cannot extend the remaining term of a patent beyond a total of 14 years from the product’s approval date. The length of the patent term extension is related to the length of time the drug, biologic or medical device is under regulatory review. It is calculated as half of the testing phase (the time between the IND submission becoming effective and the NDA, BLA or premarket approval (“PMA”) submission) and all the review phase (the time between NDA, BLA or PMA submission and approval) up to a maximum extension of five years. The time can be shortened if the FDA determines that the applicant did not pursue approval with due diligence. Only one patent applicable to an approved product is eligible for the extension, and the application for the extension must be submitted prior to the expiration of the patent. The U.S. Patent and Trademark Office (“USPTO”), in consultation with the FDA, reviews and approves the application for any patent term extension. Similar provisions are available in Europe and other foreign jurisdictions to extend the term of a patent that covers an approved drug, biologic or medical device. In the future, if any of our product candidates receive FDA approval, we expect to apply for patent term extension on patents covering those products that may be eligible for such patent term restoration.
Foreign Corrupt Practices Act
The Foreign Corrupt Practices Act (“FCPA”) prohibits any U.S. individual or business from paying, offering, or authorizing payment or offering of anything of value, directly or indirectly, to any foreign official, political party or candidate for influencing any act or decision of the foreign entity to assist the individual or business in obtaining or retaining business. The FCPA also obligates companies whose securities are listed in the U.S. to comply with accounting provisions requiring such companies to maintain books and records that accurately and fairly reflect all transactions of the corporation, including international subsidiaries, and to devise and maintain an adequate system of internal accounting controls for international operations. In Europe, and throughout the world, other countries have enacted anti-bribery laws and/or regulations similar to the FCPA.
European and Other International Government Regulation
In addition to regulations in the U.S., we will be subject to a variety of regulations in other jurisdictions governing, among other things, clinical trials and any commercial sales and distribution of our product candidates. There is no guarantee that a potential treatment will receive marketing approval or that decisions on marketing approvals or treatment indications will be consistent across geographic areas. Whether or not we obtain FDA approval for a product, we must obtain the requisite approvals from regulatory authorities in foreign countries prior to the commencement of clinical trials or marketing of the product in those countries. Some countries outside of the U.S. have a similar process to that of the FDA in that such countries require the submission of a clinical trial application (“CTA”) much like the IND prior to the commencement of human clinical trials. In Europe, for example, a CTA must typically be submitted to each country’s national health authority and an independent ethics committee, much like the FDA and an IRB. Once the CTA is approved in accordance with a country’s requirements, a clinical trial may proceed in that particular country. In the EEA, the EU Clinical Trial Regulation (“CTR”) enables sponsors since 31 January 2022 to submit one CTA via a single online platform, the Clinical Trials Information System (CTIS), to obtain approval for a clinical trial in several EEA countries.
To obtain regulatory approval to commercialize a new drug or biologic under the European Union regulatory systems, we must submit a marketing authorization application (“MAA”) with the European Medicines Agency, or “EMA”, the EEA authority in charge of medicinal products, or with a national drug approval authority. National and European Union marketing authorization procedures are similar to FDA approval procedures.
While the requirements governing the conduct of clinical trials are broadly harmonized across the EEA, in particular due to the CTR, the regulatory regimes applicable to pricing and reimbursement vary from country to country. Internationally, clinical trials are generally required to be conducted in accordance with GCP standards, applicable regulatory requirements of each jurisdiction and the medical ethics principles that have their origin in the Declaration of Helsinki.
| 30 |
Orphan Drug Status
In accordance with laws and regulations pertaining to regulatory agencies, a sponsor may request that the regulatory agencies designate a drug or biologic intended to treat a “Rare Disease or Condition” as an “Orphan Drug.” For example, in the U.S., a “Rare Disease or Condition” is defined as one which affects less than 200,000 people in the U.S., or which affects more than 200,000 people but for which the cost of developing and making available the product is not expected to be recovered from sales of the product in the U.S. Upon the approval of the first NDA or BLA for a drug or biologic designated as an Orphan Drug for a specified indication, the sponsor of that NDA or BLA is entitled to 7 years of exclusive marketing rights in the U.S. for the drug or biologic for the particular indication unless the sponsor cannot assure the availability of sufficient quantities to meet the needs of persons with the disease. In Europe, this exclusivity is 10 years. However, Orphan Drug status for an approved indication does not prevent another company from seeking approval of a drug that has other labeled indications that are not under orphan or other exclusivities. An Orphan Drug may also be eligible for federal income tax credits for costs associated with the disease state, the strength and complexity of the data presented, the novelty of the target or compound, the risk-management approval and whether multiple rounds of review are required for the agency to evaluate the submission. There is no guarantee that a potential treatment will receive marketing approval or that decisions on marketing approvals or treatment indications will be consistent across geographic areas. Our product candidate for pancreatic cancer received Orphan Drug status in the U.S. and European Union. Unlike the U.S., in the European Union, to benefit from market exclusivity, a medicine must maintain its orphan designation at the time of marketing authorization in addition to when the designation is applied.
Special FDA Expedited Review and Approval Programs
The FDA has various programs, including fast track designation, accelerated approval, priority review, and breakthrough therapy designation, which are intended to expedite or simplify the process for the development and FDA review of drugs or biologics that are intended for the treatment of serious or life-threatening diseases or conditions and demonstrate the potential to address unmet medical needs. The purpose of these programs is to provide important new drugs or biologics to patients earlier than under standard FDA review procedures.
To be eligible for a fast-track designation, the FDA must determine, based on the request of a sponsor, that a product is intended to treat a serious or life-threatening disease or condition and demonstrates the potential to address an unmet medical need. The FDA will determine that a product will fill an unmet medical need if it will provide a therapy where none exists or provide a therapy that may be potentially superior to existing therapy based on efficacy or safety factors. The FDA may review sections of the NDA or BLA for a fast-track product on a rolling basis before the complete application is submitted, if the sponsor provides a schedule for the submission of the sections of the NDA or BLA, the FDA agrees to accept sections of the NDA or BLA and determines that the schedule is acceptable, and the sponsor pays any required user fees upon submission of the first section of the NDA or BLA.
The FDA may give a priority review designation to drugs that offer major advances in treatment or provide a treatment where no adequate therapy exists. A priority review means that the goal for the FDA to review an application is six months, rather than the standard review of ten months under current PDUFA guidelines. Under the new PDUFA agreement, these six and ten-month review periods are measured from the “filing” date rather than the receipt date for NDAs for new molecular entities, which typically adds approximately two months to the timeline for review and decision from the date of submission. Most products that are eligible for fast-track designation are also likely to be considered appropriate to receive a priority review.
In addition, products tested for their safety and effectiveness in treating serious or life-threatening illnesses and that provide meaningful therapeutic benefit over existing treatments may be eligible for accelerated approval and may be approved on the basis of adequate and well-controlled clinical trials establishing that the drug product has an effect on a surrogate endpoint that is reasonably likely to predict clinical benefit, or on a clinical endpoint that can be measured earlier than irreversible morbidity or mortality, or IMM, that is reasonably likely to predict an effect on irreversible morbidity or mortality or other clinical benefit, taking into account the severity, rarity or prevalence of the condition and the availability or lack of alternative treatments. As a condition of approval, the FDA may require a sponsor of a drug receiving accelerated approval to perform post-marketing studies to verify and describe the predicted effect on IMM or other clinical endpoint, and the drug may be subject to accelerated withdrawal procedures.
| 31 |
Moreover, under the provisions of the Food and Drug Administration Safety and Innovation Act, or FDASIA, passed in July 2012, a sponsor can request designation of a product candidate as a “breakthrough therapy.” A breakthrough therapy is defined as a drug that is intended, alone or in combination with one or more other drugs, to treat a serious or life-threatening disease or condition, and preliminary clinical evidence indicates that the drug may demonstrate substantial improvement over existing therapies on one or more clinically significant endpoints, such as substantial treatment effects observed early in clinical development. Drugs designated as breakthrough therapies are also eligible for accelerated approval. The FDA must take certain actions, such as holding timely meetings and providing advice, intended to expedite the development and review of an application for approval of a breakthrough therapy.
Even if a product qualifies for one or more of these programs, the FDA may later decide that the product no longer meets the conditions for qualification or decide that the time period for FDA review or approval will not be shortened. We may explore some of these opportunities for our product candidates as appropriate.
Accelerated Approval Pathway
The FDA may grant accelerated approval to a drug for a serious or life-threatening condition that provides meaningful therapeutic advantage to patients over existing treatments based upon a determination that the drug or biologic has an effect on a surrogate endpoint that is reasonably likely to predict clinical benefit. The FDA may also grant accelerated approval for such a condition when the product has an effect on an intermediate clinical endpoint that can be measured earlier than an effect on IMM, and that is reasonably likely to predict an effect on IMM or other clinical benefit, considering the severity, rarity or prevalence of the condition and the availability or lack of alternative treatments. Drugs granted accelerated approval must meet the same statutory standards for safety and effectiveness as those granted traditional approval.
For the purposes of accelerated approval, a surrogate endpoint is a marker, such as a laboratory measurement, radiographic image, physical sign or other measure that is thought to predict clinical benefit but is not itself a measure of clinical benefit. Surrogate endpoints can often be measured more easily or more rapidly than clinical endpoints. An intermediate clinical endpoint is a measurement of a therapeutic effect that is considered reasonably likely to predict the clinical benefit of a drug, such as an effect on IMM. The FDA has limited experience with accelerated approvals based on intermediate clinical endpoints but has indicated that such endpoints generally may support accelerated approval where the therapeutic effect measured by the endpoint is not itself a clinical benefit and basis for traditional approval, if there is a basis for concluding that the therapeutic effect is reasonably likely to predict the ultimate clinical benefit of a drug.
The accelerated approval pathway is most often used in settings in which the course of a disease is long, and an extended period of time is required to measure the intended clinical benefit of a drug, even if the effect on the surrogate or intermediate clinical endpoint occurs rapidly. Thus, accelerated approval has been used extensively in the development and approval of drugs for treatment of a variety of cancers in which the goal of therapy is generally to improve survival or decrease morbidity and the duration of the typical disease course requires lengthy and sometimes large trials to demonstrate a clinical or survival benefit.
The accelerated approval pathway is usually contingent on a sponsor’s agreement to conduct, in a diligent manner, additional post-approval confirmatory studies to verify and describe the drug’s clinical benefit. As a result, a drug candidate approved on this basis is subject to rigorous post-marketing compliance requirements, including the completion of Phase 4 or post-approval clinical trials to confirm the effect on the clinical endpoint. Failure to conduct required post-approval studies, or confirm a clinical benefit during post-marketing studies, would allow the FDA to withdraw the drug from the market on an expedited basis. All promotional materials for drug candidates approved under accelerated regulations are subject to prior review by the FDA.
Under a centralized procedure in the European Union, the maximum timeframe for the evaluation of a MAA is 210 days (excluding “clock stops,” when additional written or oral information is to be provided by the applicant in response to questions asked by the Committee for Medicinal Products for Human Use (“CHMP”)). Accelerated evaluation might be granted by the CHMP in exceptional cases, for example, when a medicinal product is expected to be of a major public health interest, which takes into consideration: (i) the seriousness of the disease (e.g., heavy disabling or life-threatening diseases) to be treated; (ii) the absence or insufficiency of an appropriate alternative therapeutic approach; and (iii) anticipation of high therapeutic benefit. In this circumstance, the EMA ensures that the opinion of the CHMP is given within 150 days.
| 32 |
Healthcare Reform
The United States and many foreign jurisdictions have enacted or proposed legislative and regulatory changes affecting the healthcare system. The United States government, state legislatures and foreign governments also have shown significant interest in implementing cost-containment programs to limit the growth of government-paid healthcare costs, including price controls, restrictions on reimbursement and requirements for substitution of generic products for branded prescription drugs.
At the state level, legislatures have increasingly passed legislation and implemented regulations designed to control pharmaceutical product pricing, including price or patient reimbursement constraints, discounts, restrictions on certain product access and marketing cost disclosure and transparency measures, and, in some cases, designed to encourage importation from other countries and bulk purchasing. We expect that additional federal, state and foreign healthcare reform measures will be adopted in the future, any of which could limit the amounts that federal and state governments will pay for healthcare products and services, which could result in limited coverage and reimbursement and reduced demand for our products, once approved, or additional pricing pressures. Coverage and Reimbursement Significant uncertainty exists as to the coverage and reimbursement status of any drug products for which we obtain regulatory approval. In the U.S. and markets in other countries, sales of any products for which we receive regulatory approval for commercial sale will depend in part on the availability of reimbursement from third-party payors. Third-party payors include government health administrative authorities, managed care providers, private health insurers and other organizations. The process for determining whether a payor will provide coverage for a drug product may be separate from the process for setting the price or reimbursement rate that the payor will pay for the drug product. Third-party payors may limit coverage to specific drug products on an approved list, or formulary, which might not include all the FDA-approved drugs for a certain indication. Third-party payors are increasingly challenging the price and examining the medical necessity and cost-effectiveness of medical products and services, in addition to their safety and efficacy. We may need to conduct expensive pharmacoeconomic studies in to demonstrate the medical necessity and cost-effectiveness of our product candidates, in addition to the costs required to obtain FDA approvals. Our product candidates, if approved, may not be considered medically necessary or cost-effective. A payor’s decision to provide coverage for a drug product does not imply that an adequate reimbursement rate will be approved. Adequate third-party reimbursement may not be available to enable us to maintain price levels sufficient to realize an appropriate return on our investment in product development.
Different pricing and reimbursement schemes exist in other countries. In the European Union governments influence the price of pharmaceutical products through their pricing and reimbursement rules and control of national healthcare systems that fund a large part of the cost of those products to consumers. Some jurisdictions operate positive and negative list systems under which products may only be marketed once a reimbursement price has been agreed upon. To obtain reimbursement or pricing approval, some of these countries may require the completion of clinical trials that compare the cost-effectiveness of a product candidate to currently available therapies. Other member states allow companies to fix their own prices for medicines but monitor and control company profits. The downward pressure on healthcare costs in general, particularly prescription drugs, has become more intense.
The marketability of any product for which we receive regulatory approval for commercial sale may suffer if the government and third-party payors fail to provide adequate coverage and reimbursement. Also, an increasing emphasis on managed care in the U.S. has increased and will continue to increase the pressure on pharmaceutical pricing. Coverage policies and third-party reimbursement rates may change at any time. Even if favorable coverage and reimbursement status is attained for one or more products for which we receive regulatory approval, less favorable coverage policies and reimbursement rates may be implemented in the future.
Other U.S. Healthcare Laws and Compliance Requirements
In the U.S., our activities are potentially subject to additional regulation by various federal, state and local authorities in addition to the FDA, including the CMS, other divisions of the HHS and its Office of Inspector General, the Office for Civil Rights that has jurisdiction over matters relating to individuals’ privacy and protected health information, the DOJ, individual U.S. Attorney offices within the DOJ and state and local governments.
| 33 |
The federal Anti-Kickback Statute prohibits, among other things, knowingly and willfully offering, paying, soliciting or receiving any remuneration, directly or indirectly, to induce or in return for purchasing, leasing, ordering or arranging for the purchase, lease or order of any healthcare item or service reimbursable under Medicare, Medicaid or other federally financed healthcare program. The Anti-Kickback Statute has been interpreted broadly to proscribe arrangements and conduct where only one purpose of the remuneration between the parties was to induce or reward referrals. The term remuneration has been interpreted broadly to include anything of value. This statute has been interpreted to apply to arrangements between pharmaceutical manufacturers, on one hand, and prescribers, purchasers and formulary managers on the other. Although there are several statutory exemptions and regulatory safe harbors protecting some business arrangements from prosecution, the exemptions and safe harbors are drawn narrowly and practices that involve remuneration intended to induce prescribing, purchasing or recommending may be subject to scrutiny if they do not qualify for an exemption or safe harbor. Our practices may not in all cases meet all the criteria for safe harbor protection from federal Anti-Kickback Statute liability. Failure to meet all the requirements of an applicable safe harbor or statutory exemption, however, does not make the arrangement or conduct per se unlawful under the Anti-Kickback Statute; instead, in such cases, the legality of the arrangement would be evaluated on a case-by-case basis based on a consideration of all the facts and circumstances to ascertain the parties’ intent. Moreover, the intent standard under the Anti-Kickback Statute was amended by the Affordable Care Act to a stricter standard such that a person or entity no longer needs to have actual knowledge of the statute or specific intent to violate it to have committed a violation.
In addition, the Affordable Care Act codified case law that a claim including items or services resulting from a violation of the federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the federal False Claims Act, as discussed below. The federal Civil Monetary Penalties Law imposes penalties against any person or entity that, among other things, is determined to have presented or caused to be presented a claim to a federal health program that the person knows or should know is for an item or service that was not provided as claimed or is false or fraudulent.
The federal False Claims Act prohibits any person from knowingly presenting, or causing to be presented, a false claim for payment to the federal government or knowingly making, using or causing to be made or used a false record or statement material to a false or fraudulent claim to the federal government. Through a modification made to the Fraud Enforcement and Recovery Act of 2009, a claim includes “any request or demand” for money or property presented to the U.S. government. Pharmaceutical and other healthcare companies have been prosecuted under these laws for allegedly providing free product to customers with the expectation that the customers would bill federal programs for the product. Other companies have been prosecuted for causing false claims to be submitted because of the companies’ marketing of the product for unapproved—and thus non-reimbursable—uses.
The Federal Health Insurance Portability and Accountability Act of 1996 (“HIPAA”) created additional federal criminal statutes that prohibit knowingly and willfully executing a scheme to defraud any healthcare benefit program, including private third-party payors and knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false, fictitious or fraudulent statement in connection with the delivery of or payment for healthcare benefits, items or services. Also, many states have additional similar fraud and abuse statutes or regulations that apply to items and services reimbursed under Medicaid and other state programs, or, in several states, apply regardless of the type of payor.
In addition, we may be subject to data privacy and security regulation by both the federal government and the states in which we conduct our business. HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act (“HITECH”) and its implementing regulations, imposes requirements relating to the privacy, security and transmission of individually identifiable health information. Among other things, HITECH makes HIPAA’s privacy and security standards directly applicable to “business associates,” such as independent contractors or agents of covered entities that receive or obtain protected health information with providing a service on behalf of a covered entity. HITECH also increased the civil and criminal penalties that may be imposed against covered entities, business associates and possibly other persons. It also gave state attorneys general new authority to file civil actions for damages or injunctions in federal courts to enforce the federal HIPAA laws and seek attorney’s fees and costs associated with pursuing these actions. In addition, state laws govern the privacy and security of health information in specified circumstances, many of which differ from each other in significant ways and may not have the same effect - thus complicating compliance efforts.
| 34 |
We may be subject to other state and federal privacy laws, including laws that prohibit unfair privacy and security practices and deceptive statements about privacy and security, laws that place specific requirements on certain types of activities, such as data security and texting, and laws requiring holders of personal information to maintain safeguards and to take certain actions in response to a data breach. EEA countries, the United Kingdom, Switzerland and other jurisdictions have also adopted data protection laws and regulations, which impose significant compliance obligations.
In the EEA, the collection and use of personal data, including clinical trial data, is governed by the provisions of the General Data Protection Regulation (“GDPR”). The GDPR became effective on May 25, 2018, repealing its predecessor directive and increasing responsibility and liability of pharmaceutical and medical device companies in relation to the processing of personal data of EU data subjects. The GDPR, together with national legislation, regulations and guidelines of the EU member states governing the processing of personal data, impose strict obligations and restrictions on the ability to collect, use and transfer personal data, including health data from clinical trials and adverse event reporting. In particular, these obligations and restrictions concern the consent of the individuals to whom the personal data relates, the information provided to the individuals, the transfer of personal data out of the EEA, security breach notifications, security and confidentiality of the personal data and imposition of substantial potential fines for breaches of the data protection obligations. The United Kingdom has retained the GDPR following Brexit and supplemented it by the UK Data Protection Act 2018 (“UK GDPR”). National or local data protection laws or regulations may apply in addition to the (UK) GDPR. Furthermore, European data protection authorities may interpret the (UK) GDPR and national or local laws differently, and they may impose additional requirements, which add to the complexity of processing personal data in or from the EEA or United Kingdom. Guidance on implementation and compliance practices are often updated or otherwise revised.
The federal Physician Payments Sunshine Act under the Affordable Care Act and its implementing regulations also require that certain manufacturers of drugs, devices, biologics and medical supplies for which payment is available under Medicare, Medicaid or the Children’s Health Insurance Program, with certain exceptions, to report information related to certain payments or other transfers of value made or distributed to physicians, certain other health care professionals, and teaching hospitals, or to entities or individuals at the request of, or designated on behalf of, the physicians, health care professionals, and teaching hospitals. It also requires reporting annually certain ownership and investment interests held by physicians and their immediate family members and payments or other “transfers of value” made to such physician owners. Failure to submit timely, accurately and completely the required information may result in civil monetary penalties of up to, as adjusted in 2021, an aggregate of $189,692 per year and up to an aggregate of $1,264,622 million per year for “knowing failures”. Manufacturers were required to begin collecting data on August 1, 2013 and submit reports on aggregate payment data to the government for the first reporting period of August 1, 2013 to December 31, 2013, by March 31, 2014. They are also required to report detailed payment data for the first reporting period and submit legal attestation to the accuracy of such data by June 30, 2014. Thereafter, manufacturers must submit reports by the 90th day of each subsequent calendar year. CMS made all reported data publicly available starting on September 30, 2014. Certain states also mandate implementation of compliance programs, impose additional restrictions on pharmaceutical manufacturer marketing practices and/ or require the tracking and reporting of gifts, compensation and other remuneration to healthcare providers and entities.
Because of the breadth of these laws and the narrowness of available statutory and regulatory exemptions, it is possible that some of our business activities could be subject to challenge under one or more of such laws. If our operations are found to be in violation of any of the federal and state laws described above or any other governmental regulations that apply to us, we may be subject to penalties. These include criminal and civil monetary penalties, damages, fines, imprisonment, exclusion from participation in government programs, injunctions, recall or seizure of products, total or partial suspension of production, denial or withdrawal of pre-marketing product approvals, private “qui tam” actions brought by individual whistleblowers in the name of the government or refusal to allow us to enter supply contracts and the curtailment or restructuring of our operations. Any of these could adversely affect our ability to operate our business and our results of operations. To the extent any of our products are sold in a foreign country, we may be subject to similar foreign laws and regulations, which may include, for instance, applicable post-marketing requirements, including safety surveillance, anti-fraud and abuse laws, and implementation of corporate compliance programs and reporting of payments or transfers of value to healthcare professionals.
| 35 |
Controlled Substances Regulation
Our product candidates involving Cannabis contain controlled substances, as defined in the federal Controlled Substances Act of 1970 (“CSA”). The CSA and its implementing regulations establish a “closed system” of regulations for controlled substances. The CSA imposes registration, security, recordkeeping and reporting, storage, manufacturing, distribution, importation and other requirements under the oversight of the U.S. Drug Enforcement Administration (“DEA”). The DEA is the federal agency responsible for regulating controlled substances. It requires those individuals or entities that manufacture, import, export, distribute, research, or dispense controlled substances to comply with the regulatory requirements to prevent the diversion of controlled substances to illicit channels of commerce. The DEA categorizes controlled substances into one of five schedules—Schedule I, II, III, IV or V—with varying qualifications for listing in each schedule. Although cannabis is legal in the State of North Carolina, we had to obtain a Schedule I license for our research with our research university partner (University of Northern Colorado) that relies on federal grants. Schedule I substances have a high potential for abuse, have no currently accepted medical use in treatment in the U.S. and lack accepted safety for use under medical supervision. They may be used only in federally -approved research programs and may not be marketed or sold for dispensing to patients in the U.S. Pharmaceutical products having a currently accepted medical use that are otherwise approved for marketing may be listed as Schedule II, III, IV or V substances, with Schedule I substances presenting the highest potential for abuse and physical or psychological dependence. Schedule V substances present the lowest relative potential for abuse and dependence. The regulatory requirements are more restrictive for Schedule II substances than Schedule III substances. For example, all Schedule II drug prescriptions must be signed by a physician, physically presented to a pharmacist in most situations and cannot be refilled. Following FDA approval of a drug containing a Schedule I controlled substance, that substance must be rescheduled as a Schedule II, III, IV or V substance before it can be marketed. On November 17, 2015, H.R. 639, Improving Regulatory Transparency for New Medical Therapies Act, passed through both houses of Congress. On November 25, 2015, the bill was signed into law. The law removes uncertainty associated with timing of the DEA rescheduling process after FDA approval. Specifically, it requires DEA to issue an “interim final rule,” pursuant to which a manufacturer may market its product within 90 days of FDA approval. The law also preserves the period of orphan marketing exclusivity for the full seven years such that this period only begins after DEA scheduling. This contrasts with the previous situation whereby the orphan “clock” began to tick upon FDA approval, even though the product could not be marketed until DEA scheduling was complete.
Facilities that manufacture, distribute, import or export any controlled substance must register annually with the DEA. The DEA registration is specific to the location, activity and controlled substance schedule. For example, separate registrations are required for importation and manufacturing activities, and each registration authorizes which schedules of controlled substances the registrant may handle. However, certain coincident activities are permitted without obtaining a separate DEA registration, such as distribution of controlled substances by the manufacturer that produces them.
The DEA inspects all manufacturing facilities to review security, recordkeeping, reporting and handling prior to issuing a controlled substance registration. The specific security requirements vary by the type of business activity and the schedule and quantity of controlled substances handled. The most stringent requirements apply to manufacturers of Schedule I and Schedule II substances. Required security measures commonly include background checks on employees and physical control of controlled substances through storage in approved vaults, safes and cages, and through use of alarm systems and surveillance cameras. An application for a manufacturing registration as a bulk manufacturer for a Schedule I or II substance must be published in the Federal Register and is open for 30 days to permit interested persons to submit comments, objections or requests for a hearing. A copy of the notice of the Federal Register publication is forwarded by DEA to all those registered, or applicants for registration, as bulk manufacturers of that substance.
Once registered, manufacturing facilities must maintain records documenting the manufacture, receipt and distribution of all controlled substances. Manufacturers must submit periodic reports to the DEA of the distribution of Schedule I and II controlled substances, Schedule III narcotic substances and other designated substances. Registrants must also report any controlled substance thefts or significant losses and must obtain authorization to destroy or dispose of controlled substances. As with applications for registration as a bulk manufacturer, an application for an importer registration for a Schedule I or II substance must also be published in the Federal Register, which remains open for 30 days for comments. Imports of Schedule I and II controlled substances for commercial purposes are generally restricted to substances not already available from domestic supplier or where there is not adequate competition among domestic suppliers. In addition to an importer or exporter registration, importers and exporters must obtain a permit for every import or export of a Schedule I and II substance or Schedule III, IV and V narcotic, and submit import or export declarations for Schedule III, IV and V non-narcotics. In some cases, Schedule III non-narcotic substances may be subject to the import/export permit requirement, if necessary, to ensure that the U.S. complies with its obligations under international drug control treaties.
| 36 |
For drugs manufactured in the U.S., the DEA establishes annually an aggregate quota for substances within Schedules I and II that may be manufactured or produced in the U.S. based on the DEA’s estimate of the quantity needed to meet legitimate medical, scientific research and industrial needs. This limited aggregate amount of Cannabis that the DEA allows to be produced in the U.S. each year is allocated among individual companies, which, in turn, must annually apply to the DEA for individual manufacturing and procurement quotas. The quotas apply equally to the manufacturing of the active pharmaceutical ingredient and production of dosage forms. The DEA may adjust aggregate production quotas and individual manufacturing or procurement quotas from time to time during the year, although the DEA has substantial discretion in whether to make such adjustments for individual companies.
The states also maintain separate controlled substance laws and regulations, including licensing, recordkeeping, security, distribution and dispensing requirements. State authorities, including boards of pharmacy, regulate use of controlled substances in each state. Failure to maintain compliance with applicable requirements, particularly as manifested in the loss or diversion of controlled substances, can result in enforcement action that could have a material adverse effect on our business, operations and financial condition. The DEA may seek civil penalties, refuse to renew necessary registrations, or initiate proceedings to revoke those registrations. In certain circumstances, violations could lead to criminal prosecution.
Patents, Intellectual Property and Trade Secrets
Intellectual property and patent protection are of paramount importance to our business, as are the trade secrets and other strategies we have employed with Austrianova to protect the proprietary Cell-in-a-Box® technology. Although we believe we take reasonable measures to protect our intellectual property and trade secrets and those of Austrianova, we cannot guarantee we will be able to protect and enforce our IP or obtain patent protection for our product candidates as needed. We license technology and trademarks relating to three areas: (i) live cell encapsulation with cells that express cytochrome P450 where the capsule is permeable to prodrug molecules and the cells are retained within the capsules; (ii) treatment of solid cancerous tumors and (ii) encapsulation of cells for producing retroviral particles for gene therapy. We also have exclusive licensing rights to patents, trademarks and know-how using Cell-in-a-Box® technology in the diabetes field and in the treatment of diseases and related conditions using cannabinoids.
Litigation may be required to protect our product candidates, intellectual property rights or to determine the validity and scope of the proprietary rights of others. Establishment, maintenance and enforcement of our intellectual property utilizes financial and operational resources. In addition, the possibility exists that our intellectual property could be discovered to be owned by others, be invalid or be unenforceable - potentially bringing unforeseen challenges to us.
Intellectual Property Agreements
The following agreements are a material component of our intellectual property:
| · | We are a party to the Bavarian Nordic/GSF License Agreement pursuant to which Bavarian Nordic/GSF are the licensors and Bio Blue Bird, our wholly owned subsidiary, is the licensee. The Bavarian Nordic/GSF License Agreement was signed in July 2005 and amended in December 2006. Pursuant to the Bavarian Nordic/GSF License, the licensee is granted an exclusive license to use Bavarian Nordic’s clinical data and know-how for encapsulating genetically modified human cells to treat cancer. The licensors have rights to terminate the license if the annuity and upkeep fees are not paid to Bavarian Nordic, there is not proper reporting or there is not a clearly documented effort to commercialize this technology. The term of the Bavarian Nordic/GSF License Agreement expired on March 27, 2017. | |
| · | In October 2016, Bavarian Nordic/GSF and Bio Blue Bird amended the Bavarian Nordic/GSF License Agreement to include, among other things, the right to import within the scope of the license, reflect ownership and notification of improvements, clarify which provisions survive expiration or termination of the Bavarian Nordic License Agreement and provide rights to Bio Blue Bird to the clinical data and know-how after the expiration of the licensed patent rights. | |
| · | The Diabetes Licensing Agreement provides us with an exclusive worldwide license, with a right to sublicense, to use the Cell-in-a-Box® trademark and its associated technology with genetically modified or non-modified non-stem cell lines and induced pluripotent stem (“iPS”) cells designed to produce insulin or other critical components for the treatment of diabetes. |
| 37 |
| · | The Cannabis Licensing Agreement provides us with an exclusive worldwide license, with a right to sublicense, to use the Cell-in-a-Box® trademark and its associated technology with genetically modified non-stem cell lines which are designed to convert cannabinoids to their active form to develop therapies for diseases and their related symptoms. | ||
|
|
· | We entered into a Binding Term Sheet with SG Austria and Austrianova pursuant to which the parties reached an agreement to amend certain provisions in the SG Austria APA, the Diabetes Licensing Agreement and the Cannabis Licensing Agreement. | |
| · | We entered into the amendments contemplated by the Binding Term Sheet Amendments. The Binding Term Sheet Amendments provide that our obligation to make milestone payments to Austrianova will be eliminated in their entirety under the: (i) Cannabis License Agreement; and (ii) the Diabetes License Agreement, as amended. The Binding Term Sheet Amendments also provides that our obligation to make milestone payments to SG Austria pursuant to the SG Austria APA, as amended and clarified, is eliminated in their entirety. One of the Binding Term Sheet Amendments also provides that the scope of the Diabetes License Agreement is expanded to include all cell types and cell lines of any kind or description now or later identified, including, but not limited to, primary cells, mortal cells, immortal cells and stem cells at all stages of differentiation and from any source specifically designed to produce insulin for the treatment of diabetes. | ||
| · | In addition, one of the Binding Term Sheet Amendments provides that we have a 5-year right of first refusal from August 30, 2017 in the event that Austrianova chooses to sell, transfer or assign at any time during this period the Cell-in-a-Box® technology, tradename and Associated Technologies; provided, however, that the Associated Technologies subject to the right of first refusal do not include Bac-in-a-Box. | ||
| · | The Binding Term Sheet Amendments further provide that: (i) the royalty payments on gross sales as specified in the SG Austria APA, the Cannabis License Agreement and the Diabetes License Agreement are changed to 4%; and (ii) the royalty payments on amounts received by us from sublicensees on sublicensees’ gross sales under the same agreements are changed to 20% of the amount received by us from our sublicensees, provided, however, that in the event the amounts received by us from sublicensees is 4% or less of sublicensees’ gross sales, Austrianova will receive 50% of what we receive (up to 2%) and then additionally 20% of any amount we receive over that 4%. | ||
| · | The Binding Term Sheet Amendments also provide that Austrianova will receive 50% of any other financial and non-financial consideration received from our sublicensees of the Cell-in-a-Box® technology. | ||
| · |
The Melligen Cell License Agreement provides us with an exclusive worldwide license, with a right to sublicense, to use genetically modified human cells that have been modified to comprise pancreas islet cell glucokinase for use in developing a therapy for diabetes. The Melligen cells are patent protected in the U.S. and Europe, which expire in August 2028, subject to any applicable patent term adjustment or extension that may be available. | ||
Material Agreements
Third Addendum to the SG Austria APA
In June 2013, we and SG Austria entered the Third Addendum and the Clarification Agreement. The Third Addendum requires us to make the following payments for the purchased assets; these payments were timely made in full under the payment deadlines set forth in the Third Addendum:
| · | A $60,000 payment due under the SG Austria APA; | |
| · | A payment of Stamp Duty estimated to be $10,000-17,000 to the Singapore Government; | |
| · | $500,000 to be used to pay off the existing debt of Bio Blue Bird; and | |
| · | $1,000,000 to SG Austria. |
| 38 |
Pursuant to the Third Addendum, we agreed to and have entered a manufacturing agreement with SG Austria for the manufacture of the pancreatic cancer clinical trial product to treat LAPC. The Manufacturing Framework Agreement requires us to pay Austrianova a one-time manufacturing setup fee in the amount of $647,000, of which 50% is required to be paid on the effective date of the Manufacturing Framework Agreement and 50% is required to be paid three months later. We have paid the full amount of the manufacturing setup fee.
The Manufacturing Framework Agreement also requires us to pay a fee for producing the final encapsulated cell product of $647 per vial of 300 capsules after production, with a minimum purchased batch size of 400 vials of any Cell-in-a-Box® product. The fees under the Manufacturing Framework Agreement are subject to annual increases according to the annual inflation rate in the country in which the encapsulated cell products are manufactured. We placed and have received an order to produce 400 vials for our clinical trial to treat LAPC. Austrianova has been paid the full amount for the order.
The Third Addendum also requires the Company to make future royalty and milestone payments as follows:
| · | Two percent royalty on all gross sales received by us or our affiliates; | |
| · | Ten percent royalty on gross revenues received by us or our affiliates from a sublicense or right to use the patents or the licenses granted by us or our affiliates; | |
| · | Milestone payments of $100,000 within 30 days after enrollment of the first human patient in the first clinical trial for each product; $300,000 within 30 days after enrollment of the first human patient in the first Phase 3 clinical trial for each product; and $800,000 within 60 days after having a NDA or a BLA approved by the FDA or a MAA approved by the EMA in Europe, or its equivalent based on the country in which it is accepted for each product; and | |
| · | Milestone payments of $50,000 due 30 days after enrollment of the first veterinary patient in the first trial for each product and $300,000 due 60 days after having a BLA, a NDA or a MAA or its equivalent approved based on the country in which it is accepted for each veterinary product. |
On May 14, 2018, we entered into amendments to the Third Addendum. For a full description of these amendments, see Item 1. “History of the Business.”
Diabetes Licensing Agreement
Under the Diabetes Licensing Agreement, we are required to make a payment of $2,000,000 in two equal payments of $1,000,000 each. We made our first $1,000,000 payment on October 30, 2013. Our second payment of $1,000,000 was made on February 25, 2014.
The Diabetes Licensing Agreement requires us to pay Austrianova, pursuant to a manufacturing agreement to be entered between the parties, a one-time manufacturing setup fee in the amount of approximately $600,000, of which 50% is required to be paid on the signing of a manufacturing agreement for a product and 50% is required to be paid three months later. In addition, the Diabetes Licensing Agreement requires us to pay a manufacturing production fee, which is to be defined in the manufacturing agreement, for producing the final encapsulated cell product of approximately $600.00 per vial of 300 capsules after production, with a minimum purchased batch size of 400 vials of any Cell-in-a-Box® encapsulation-based product. All costs for encapsulated cell products will be subject to an annual increase equal to the published rate of inflation in the country of manufacture of the vials.
| 39 |
The Diabetes Licensing Agreement requires us to make future royalty and milestone payments as follows:
| · | Ten percent royalty of gross sales of all products we sell; | |
| · | Twenty percent royalty of the amount received by us from a sub-licensee on its gross sales; and | |
| · | Milestone payments of $100,000 within 30 days of beginning the first pre-clinical experiments using the encapsulated cells; | |
| · | $500,000 within 30 days after enrollment of the first human patient in the first clinical trial; $800,000 within 30 days after enrollment of the first human patient in the first Phase 3 clinical trial and; | |
| · | $1,000,000 within 90 days after having a NDA or a BLA approved by the FDA or a MAA approved by the EMA in Europe, or its equivalent based on the country in which it is accepted for each product. |
The license under the Diabetes Licensing Agreement, as amended, may be terminated and all rights will revert to Austrianova if any of the following milestone events do not occur within the following timeframes, subject to all the necessary and required research having been successful and the relevant product being sufficiently prepared to enter a clinical trial:
| · | If we fail to enter a research program with the technology in the scope of the license providing a total funding equal to or greater than $400,000 within three years of June 25, 2013, the effective date of the Diabetes Licensing Agreement (we have met this requirement); or | |
| · | If we fail to enter a clinical trial or its equivalent for a product within seven years of the effective date of the Diabetes Licensing Agreement. |
In May 2018, we entered into amendments to the Diabetes Licensing Agreement. For a full description of these amendments, see Item 1. “History of the Business.”
Cannabis Licensing Agreement
Pursuant to the Cannabis Licensing Agreement, we acquired from Austrianova an exclusive worldwide license to use the Cell-in-a-Box® trademark and its associated technology with genetically modified non-stem cell lines which are designed to activate cannabinoids to develop therapies involving Cannabis with a right to sublicense.
Under the Cannabis Licensing Agreement, we are required to pay Austrianova an initial upfront payment of $2,000,000 (“Upfront Payment”). We have the right to make periodic monthly partial payments of the Upfront Payment in amounts to be agreed upon between the parties prior to each such payment being made. Under the Cannabis Licensing Agreement, the Upfront Payment must be paid in full by no later than June 30, 2015. The parties amended the Cannabis Licensing Agreement twice pursuant to which the balance of the Upfront Payment is to be paid by June 30, 2016. We have paid the Upfront Payment of $2,000,000 in full.
The Cannabis Licensing Agreement requires us to pay Austrianova, pursuant to a manufacturing agreement to be entered between the parties, a one-time manufacturing setup fee in the amount of $800,000, of which 50% is required to be paid on the signing of a manufacturing agreement for a product and 50% is required to be paid three months later. In addition, the Cannabis Licensing Agreement requires us to pay a manufacturing production fee, which is to be defined in the manufacturing agreement, for producing the final encapsulated cell product of $800 per vial of 300 capsules after production with a minimum purchased batch size of 400 vials of any Cell-in-a-Box® product. All costs for encapsulated cell products, the manufacturing setup fee and the manufacturing production fee will be subject to annual increases, in accordance with the inflation rate in the country in which the encapsulated cell products are manufactured.
| 40 |
The Cannabis Licensing Agreement requires us to make future royalty and milestone payments as follows:
| · | Ten percent royalty of the gross sale of all products sold by us; | |
| · | Twenty percent royalty of the amount received by us from a sublicense on its gross sales; and | |
| · | Milestone payments of $100,000 within 30 days of beginning the first pre-clinical experiments using the encapsulated cells; $500,000 within 30 days after enrollment of the first human patient in the first clinical trial; $800,000 within 30 days after enrollment of the first human patient in the first Phase 3 clinical trial; and $1,000,000 within 90 days after having a NDA or a BLA approved by the FDA or a MAA approved by the EMA or its equivalent based on the country in which it is accepted for each product. |
The license under the Cannabis Licensing Agreement, as amended, may be terminated and all rights will revert to Austrianova if any of the following milestone events do not occur within the following timeframes:
| · | If we do not enter a research program involving the scope of the license within three years of December 1, 2014, the effective date of the Cannabis Licensing Agreement (we have met this requirement); or | |
| · | If we do not enter a clinical trial or its equivalent for a product within 7 years of the effective date of the Cannabis Licensing Agreement. |
In May 2018, we entered into amendments to the Cannabis Licensing Agreement. For a full description of these amendments, see Item 1. “History of the Business.”
Melligen Cell License Agreement
The Melligen Cell License Agreement requires that we pay royalty, milestone and patent costs to UTS as follows:
| · | Six percent of gross exploitation revenue on product sales; | |
| · | Twenty-five percent of gross revenues if the product is sublicensed by us; | |
| · | Milestone payments of AU$ 50,000 at the successful conclusion of a preclinical study, AU$ 100,000 at the successful conclusion of a Phase 1 clinical trial, AU$ 450,000 at the successful conclusion of a Phase 2 clinical trial, and AU$ 3,000,000 at the successful conclusion of a Phase 3 clinical trial; and | |
| · | Patent costs of fifteen percent of the costs paid by UTS to prosecute and maintain patents related to the licensed intellectual property. |
In the event of a default under the Melligen Cell License Agreement, the non-defaulting party may immediately terminate the agreement by notice in writing to the defaulting party if: (i) the default has continued for not less than 14 days or occurred more than 14 days earlier and has not been remedied; (ii) the non-defaulting party serves upon the defaulting party notice in writing requiring the default to be remedied within 30 days of such notice, or such greater number of days as the non-defaulting party may in its discretion allow, and (iii) the defaulting party has failed to comply with the notice referred to in (ii) above.
The Melligen Cell License Agreement was amended in April 2016 to change the name of the licensee to our current name and clarify certain ambiguities in the agreement. We are required to pay the Melligen cell patent prosecution costs and to pay to UTS a patent administration fee equal to 15% of all amounts paid by UTS to prosecute and maintain patents related to the Melligen cells.
In August 2017, we entered into the Binding Term Sheet pursuant to which the parties reached an agreement to amend certain provisions in the SG Austria APA, the Diabetes Licensing Agreement and the Cannabis Licensing Agreement.
In May 2018, we entered into agreements with SG Austria and Austrianova to amend certain provisions of the SG Austria APA, the Diabetes Licensing Agreement and the Cannabis Licensing Agreement pursuant to the Binding Term Sheet. For a full description of these amendments, see Item 1. “History of the Business.”
| 41 |
Sources and Availability of Raw Materials
The entire encapsulation process relating to the encapsulation of the cells for the oncology and diabetes-based therapies we are developing is to be carried out by Austrianova. Austrianova is the sole source of our product candidates. Austrianova is responsible for acquiring all of the necessary raw materials used in this process, including the cellulose sulfate necessary for encapsulating the live cells. Austrianova from time to time has experienced significant supply chain delays, some of which may be related to COVID-19. We believe Austrinova may also be experiencing liquidity issues. Those cells have been grown by Eurofins to populate a MCB for our future clinical trials. See also “—Manufacturing” in this Item 1. “Business.”
Employees
As of April 30, 2022, we had 4 full-time employees and 23 consultants who devote substantial time to us. The consultants are physicians, scientists, regulatory experts, clinical operation experts and cGMP experts. All of our research and development (“R&D”) work is handled by our consultants.
Recent Developments
We recently received notice from Iroquois Capital Management, LLC and certain of its affiliates nominating a slate of eight individuals for election to our Board of Directors for the 2022 annual meeting. If a proxy contest or consent solicitation results from this notice, our business could be adversely affected because: (i) responding to proxy contests and other actions by activist shareholders can be costly and time-consuming, which could disrupt our operations and divert the attention of management and our employees; (ii) perceived uncertainties as to our future direction could adversely affect our relationships with customers, suppliers, investors, prospective and current team members and others, resulting in the loss of potential business opportunities, or making it more difficult to attract and retain qualified personnel; and (iii) if individuals are elected to our Board of Directors with a specific agenda, it may adversely affect our ability to effectively and timely implement our strategic plan. These actions could also cause our stock price to experience periods of volatility. In addition, future proxy contests and other actions by activist shareholders could require us to incur significant legal fees and solicitation expenses and require significant time and attention by management and the Board of Directors and could materially and adversely affect our business and operating results. We may also be subject, from time to time, to other legal and business challenges in the operation of our company due to actions instituted by activist shareholders. Responding to such actions could be costly and time-consuming.
Medical and Scientific Advisory Board
We regularly seek advice and input from the members of our Medical and Scientific Advisory Board on matters related to our R&D programs. The members of our Medical and Scientific Advisory Board consist of experts across a wide range of key disciplines relevant to our clinical development programs. We intend to continue to leverage the broad expertise of our advisors by seeking their counsel on important topics relating to our product development and clinical development programs. The members of our Medical and Scientific Advisory Board are not our employees and may have commitments to, or consulting or advisory contracts with, other entities that may limit their availability to us. In addition, our advisors may have arrangements with other companies to assist those companies in developing products or other technologies. All the members of our Medical and Scientific Advisory Board are affiliated with other entities and devote only a portion of their time to us. The members of our Medical and Scientific Advisory Board are not officers or directors of our company. Our current advisors are:
| · | Dr. Manuel Hidalgo – Chief of the Division of Hematology and Medical Oncology at Weill Cornell Medicine and New York-Presbyterian/Weill Cornell Medical Center in New York, New York; | |
| · | Dr. Brian Salmons – Chief Executive Officer and President of Austrianova and Co-Developer of Cell-in-a-Box® and its Associated Technologies; | |
| · | Dr. Mark L. Rabe – former Chief Executive Officer of Rabe Medical Solutions, San Diego, California; and | |
| · | David A. Judd - cellular biologist for 35 years and a long-term employee of the Grand Island Biological Company with experience in culturing various types of human cells, including the cells that were transfected with the gene that activates the prodrug ifosfamide and that are encapsulated for our LAPC clinical trial. |
| 42 |
Financial Information Concerning Geographic Areas
We had no revenues in the fiscal years ended April 30, 2022, and 2021, including no revenues from foreign countries. We have long-lived assets, other than financial instruments, located in the following geographical areas:
| FY 2022 | FY 2021 | |||||||
| United States: | $ | 5,129,308 | $ | 5,128,992 | ||||
| All foreign countries, in total: | $ | 0 | $ | 0 | ||||
We operate globally and are attempting to develop products in multiple countries. Consequently, we face complex legal and regulatory requirements in multiple jurisdictions, which may expose us to certain financial and other risks. International operations are subject to a variety of risks, including:
| · | foreign currency exchange rate fluctuations; | |
| · | greater difficulty in overseeing foreign operations; | |
| · | logistical and communications challenges; | |
| · | potential adverse changes in laws and regulatory practices, including export license requirements, trade barriers, tariffs and tax laws; | |
| · | burdens and costs of compliance with a variety of foreign laws; | |
| · | political and economic instability; | |
| · | increases in duties and taxation; | |
| · | foreign tax laws and potential increased costs associated with overlapping tax structures; | |
| · | greater difficulty in protecting intellectual property; | |
| · | the risk of third-party disputes over ownership of intellectual property and infringement of third-party intellectual property by our product candidates; | |
| · | risks resulting from our extensive supply chain exposure to Asia; and | |
| · | general social, economic and political conditions in these foreign markets. |
We are dependent on business relationships with parties in multiple countries, as disclosed in Item 1A. “Risk Factors—Risks Related to Our Dependence on Third Parties.”
Our Corporate Information
We are a Nevada corporation incorporated in 1996. In 2013, we restructured our operations to focus on biotechnology. The restructuring resulted in us focusing all of our efforts developing a novel, effective and safe way to treat cancer and diabetes. In January 2015, we changed our name from Nuvilex, Inc. to PharmaCyte Biotech, Inc. to reflect the nature of our current business.
Our corporate headquarters are located at 3960 Howard Hughes Parkway, Suite 500, Las Vegas, Nevada 89169. Our telephone number is (917) 595-2850. We maintain a website at www.pharmacyte.com to which we post copies of our press releases as well as additional information about us. Our filings with the SEC are available free of charge through our website as soon as reasonably practicable after being electronically filed with or furnished to the SEC. Information contained in our website is not a part of, nor incorporated by reference into, this Report or our other filings with the SEC, and should not be relied upon.
| 43 |
ITEM 1A. RISK FACTORS
You should carefully consider these factors that may affect future results, together with all the other information included in this Report in evaluating our business. The risks and uncertainties described below are those that we currently believe may materially affect our business and results of operations. Additional risks and uncertainties that we are unaware of or that we currently deem immaterial also may become important factors that affect our business and results of operations. Our shares of common stock involve a high degree of risk and should be purchased only by investors who can afford a loss of their entire investment. Prospective investors should carefully consider the following risk factors concerning our business before making an investment.
In addition, you should carefully consider these risks when you read “forward-looking” statements elsewhere in this Report. These are statements that relate to our expectations for future events and time periods. Generally, the words “anticipate,” “expect,” “intend,” and similar expressions identify forward-looking statements. Forward-looking statements involve risks and uncertainties, and future events and circumstances could differ significantly from those anticipated in the forward-looking statements.
Forward-Looking Statements and Associated Risks
We operate in a competitive and rapidly changing environment. New risks emerge from time to time. It is not possible for us to predict all of those risks, nor can we assess the impact of all of those risks on our business or the extent to which any factor may cause actual results to differ materially from those contained in any forward-looking statement. The forward-looking statements in this Report are based on assumptions management believes are reasonable. However, due to the uncertainties associated with forward-looking statements, you should not place undue reliance on any forward-looking statements. Further, forward-looking statements speak only as of the date they are made, and unless required by law, we expressly disclaim any obligation or undertaking to publicly update any of them in light of new information, future events, or otherwise.
Summary of Risks Associated with Our Business
Our business is subject to numerous risks and uncertainties that you should consider before investing in our company. These risks are described more in more detail in the section titled “Risk Factors” in Item 1A of this Report. These risks include, but are not limited to, the following:
| · | We are a biotechnology company with limited resources, a limited operating history and no products approved for clinical trials or commercial sale, which may make it difficult to evaluate our current business and predict our future success and viability. |
| · | As a result of the clinical hold that has been placed on our IND by the FDA, it has taken and may continue to take considerable time and expense to respond to the FDA, and no assurance can be given that the FDA will remove the clinical hold in which case our business and prospects will likely suffer material adverse consequences. |
| · | We contract with Austrianova for the manufacture of our product candidates for preclinical studies and clinical trials, if allowed to proceed, and expect to continue to do so for commercialization. This reliance on Austrianova increases the risk that we will not have sufficient quantities of our product candidates or such quantities at an acceptable cost, which could delay, prevent or impair our development or commercialization efforts. |
| · | Disruptions in the global economy and supply chains may have a material adverse effect on our business, financial condition and results of operations and the financial condition of the third parties on which we rely, including Austrianova. |
| · | Our business could be impacted as a result of actions by activist shareholders, including as a result of a potential proxy contest for the election of directors at our 2022 annual meeting. |
| · | The recent and ongoing COVID-19 pandemic has affected and could continue to affect our operations, as well as the business or operations of third parties with whom we conduct business. Our business could be adversely affected by the effects of other future health pandemics in regions where we or third parties on which we rely have significant business operations. |
| 44 |
| · | If we are unable to successfully raise additional capital in addition to our recent completed public offering, our future clinical trials and product development could be limited, and our long-term viability may be threatened. |
| · | Due to the significant resources required for the development of our programs, and depending on our ability to access capital, we must prioritize development of certain product candidates. We may expend our limited resources on programs that do not yield a successful product candidate and fail to capitalize on product candidates or indications that may be more profitable or for which there is a greater likelihood of success. |
| · | We currently have no commercial revenue and may never become profitable. |
| · | If we are unable to obtain, or if there are delays in obtaining, required approval from the applicable regulatory agencies, we will not be able to commercialize our product candidates and our ability to generate revenue will be materially impaired. |
| · | If allowed to proceed with our clinical development program, we intend to conduct clinical trials for certain of our product candidates at sites outside of the U.S., and the U.S. regulatory agencies may not accept data from trials conducted in such locations. |
| · | Promising results in previous clinical trials of our encapsulated live cell and ifosfamide combination for advanced pancreatic cancer may not be replicated in future clinical trials which could result in development delays or a failure to obtain marketing approval. |
| · | We may not be able to protect our intellectual property rights throughout the world. |
| · |
We rely and expect to continue to rely heavily on third parties to conduct our preclinical studies, plan to rely on third parties to conduct our and clinical trials, assuming they are allowed to proceed, and those third parties may not perform satisfactorily, including failing to meet deadlines for the completion of such studies and trials.
| |
| · | Disruptions in the global economy and supply chains may have a material adverse effect on our business, financial condition and results of operations and the financial condition of the third parties on which we rely, including Austrianova. |
| · | Our business could be impacted as a result of actions by activist shareholders, including as a result of a potential proxy contest for the election of directors at our annual meeting. |
| · | You may experience future dilution as a result of future equity offerings. | |
| · | If we fail to comply with the continuing listing standards on Nasdaq, our securities could be delisted which could limit investors’ ability to make transactions in our securities and subject us to additional trading restrictions. |
| · | We may experience volatility in our stock price, which may adversely affect the trading price of our common stock. |
| · | A large number of shares may be issued and subsequently sold upon the exercise of existing options and warrants. |
| · | We are a “smaller reporting company” under the SEC’s disclosure rules and have elected to comply with the reduced disclosure requirements applicable to smaller reporting companies. |
| · | As a non-accelerated filer, we are not required to comply with the auditor attestation requirements of the Sarbanes-Oxley Act. |
| 45 |
Risks Related to Our Financial Position, FDA Clinical Hold, Need for Additional Capital and Overall Business
We are a biotechnology company with limited resources, a limited operating history, and no products approved for clinical trials or commercial sale, which may make it difficult to evaluate our current business and predict our future success and viability.
We are a biotechnology company focused on developing cellular therapies for cancer based upon a proprietary cellulose-based live cell encapsulation technology known as “Cell-in-a-Box®.” In recent years, we have devoted substantially all our resources to the development of our product candidates for LAPC. We have limited resources, a limited operating history, no products approved for clinical trials or commercial sale and therefore have not produced any revenues. We have generated significant operating losses since our inception. Our net losses for the years ended April 30, 2022, and 2021 were approximately $4.2 million and $3.6 million, respectively. As of April 30, 2022, we had an accumulated deficit of approximately $112 million. Substantially all our losses have resulted from expenses incurred relating to our research and development programs and from general and administrative expenses and operating losses associated with our business.
We expect to continue to incur significant expenses and operating losses for the foreseeable future. We anticipate these losses will increase as we continue our research and development of, and, if approved by the FDA, commence clinical trials for, our product candidates. In addition to budgeted expenses, we may encounter unforeseen expenses, difficulties, complications, delays and other unknown factors that may adversely affect our business.
We have no facilities to conduct fundamental research and we have performed our research and development activities by collaboration with contract service providers, and contract manufacturers and by designing and developing research programs in collaboration with university-based experts who work with us to evaluate mechanism(s) of disease for which we have designed and developed product candidates. We have not maintained a principal laboratory or primary research facility for the development of our product candidates.
Biotechnology product development is a highly uncertain undertaking and involves a substantial degree of risk. We have not commenced or completed clinical trials for any of our product candidates, obtained marketing approval for any product candidates, manufactured a commercial scale product, or arranged for a third party to do so on our behalf, or conducted sales and marketing activities necessary for successful product commercialization. Given the highly uncertain nature of biotechnology product development, we may never commence or complete clinical trials for any of our product candidates, obtain marketing approval for any product candidates, manufacture a commercial scale product or arrange for a third party to do so on our behalf, or conduct sales and marketing activities necessary for successful product commercialization.
Our limited operating history as a company makes any assessment of our future success and viability subject to significant uncertainty. We will encounter risks and difficulties frequently experienced by early-stage biotechnology companies in rapidly evolving fields, and we have not yet demonstrated an ability to successfully overcome such risks and difficulties. If we do not address these risks and difficulties successfully, our business, operating results and financial condition will suffer.
As a result of the clinical hold that has been placed on our IND by the FDA, it has taken and may continue to take considerable time and expense to respond to the FDA and no assurance can be given that the FDA will remove the clinical hold in which case our business and prospects will likely suffer material adverse consequences.
On October 1, 2020, we received notice from the FDA that it had placed our IND for a planned Phase 2b clinical trial in LAPC on clinical hold. As part of the clinical hold process, the FDA has asked for additional information, tasks to be performed by us and new preclinical studies and assays. It has taken and may continue to take a considerable period of time, the length of which is not certain at this time, for us to conduct such tasks and preclinical studies and to generate and prepare the requested information. It is possible that the service providers that we will utilize for such work may have considerable backlogs and/or are suffering from slowdowns as a result of COVID-19 and supply chain disruptions and may not be able to perform such work for an extended period of time. Even if we are able to fully respond to the FDA’s requests, they may subsequently make additional requests that we would need to fulfill prior to the lifting of the clinical hold and we may never be able to begin our clinical trial in LAPC, obtain regulatory approval or successfully commercialize our product candidates. An inability to conduct our clinical trial in LAPC as a result of the clinical hold or otherwise, would likely force us to terminate our clinical development plans. It is possible that we will be unable to fully respond to the FDA in a satisfactory manner, and as a result the clinical hold may never be lifted. If the clinical hold is not lifted or if the lifting takes an extended period of time, our business and prospects will likely suffer material adverse consequences.
| 46 |
We contract with Austrianova for the manufacture of our product candidates for preclinical studies and clinical trials, if allowed to proceed, and expect to continue to do so for commercialization. This reliance on Austrianova increases the risk that we will not have sufficient quantities of our product candidates or such quantities at an acceptable cost, which could delay, prevent or impair our development or commercialization efforts.
We do not currently own or operate manufacturing facilities to produce our encapsulated live cell product candidates for cancer, diabetes and malignant ascites. We rely on and expect to continue to rely on Austrianova to manufacture supplies of our product candidates for preclinical studies and clinical trials, if allowed to proceed, as well as for commercial manufacture of our product candidates, and these must be maintained for us to receive marketing approval for our product candidates.
Our encapsulated live cell product candidates must be manufactured through complex, multi-step synthetic processes that are time-consuming and involve special conditions at certain stages. Biologics and drug substance manufacture requires high potency containment, and containment under aseptic conditions. Any performance failures on the part of our existing or future manufacturers could delay clinical development or marketing approval of our product candidates. Moreover, the facilities that produce our Cell-in-a-Box® capsules are unique to us and would not be replicable or replaceable promptly, if at all, if those facilities become unavailable or are damaged or destroyed through an accident, natural disaster, labor disturbance or otherwise.
If Austrianova should become unavailable to us for any reason, we may incur additional cost or delay in identifying or qualifying a replacement manufacturer. At this time, we are unaware of any available substitute manufacturer other than Austrianova. In addition, while we believe that our existing manufacturer, Austrianova, can produce our product candidates, if approved, in commercial quantities, we may also need to identify a third-party manufacturer capable of providing commercial quantities of our product candidates. If we are unable to arrange for such a third-party manufacturing source or fail to do so on commercially reasonable terms and in a timely manner, we may not be able to successfully produce and market our encapsulated live cell and ifosfamide product or any other product candidate or may be delayed in doing so.
Even if we can establish such arrangements with another third-party manufacturer, reliance on a new third-party manufacturer entails additional risks, including:
| · | Reliance on the third party for regulatory compliance and quality assurance; | |
| · | The possible breach of the manufacturing agreement by the third party; | |
| · | The possible misappropriation of our proprietary information, including our trade secrets and know-how; and | |
| · | The possible termination or nonrenewal of the agreement by the third party at a time that is costly or inconvenient for us. |
A new third-party manufacturer may not be able to comply with cGMP standards or the requirements of a regulatory agency. Our failure, or the failure of our third-party manufacturer, to comply with these practices or requirements could result in sanctions being imposed on us, including additional clinical holds, fines, injunctions, civil penalties, delays, suspension or withdrawal of approvals, license revocation, seizures or recalls of product candidates or products, operating restrictions and criminal prosecutions, any of which could significantly and adversely affect supplies of our product candidates.
Delays in the cGMP certification of the Austrianova manufacturing facility in Bangkok, Thailand could affect its ability to manufacture encapsulated live cells on a timely basis and could adversely affect supplies of our product candidates for clinical trials and to market.
Our product candidates that we may develop may compete with other product candidates and products for access to manufacturing facilities. There are a limited number of manufacturers that operate under cGMP regulations and that might be capable of manufacturing products for us.
| 47 |
In addition, we expect to rely on Austrianova to purchase from third-party suppliers the materials necessary to produce our product candidates for our clinical studies, if allowed to proceed. There are a small number of suppliers for certain equipment and raw materials that are used in the manufacture of our product candidates. Such suppliers may not sell these raw materials to Austrianova at the times we need them or on commercially reasonable terms. For example, there is from time to time a limited supply of acceptable cell media for production of our MCB. We do not have any control over the process or timing of the acquisition of these raw materials by Eurofins or Austrianova. Moreover, we currently do not have any agreements for the commercial production of these raw materials. Austrianova from time to time has experienced significant supply chain disruptions, some of which may be related to COVID-19, and we believe it is experiencing liquidity issues. Any further significant delay in the supply of a product candidate or the raw material components thereof our clinical trials, if allowed to proceed, due to the need to replace a third-party supplier of these raw materials could considerably delay completion of our clinical studies, product testing and potential regulatory approval of our product candidates. If Eurofins, Austrianova or we are unable to purchase these raw materials after regulatory approval has been obtained for our product candidates, the commercial launch of our product candidates would be delayed or there would be a shortage in supply, which would impair our ability to generate revenues from the sale of our product candidates.
Our current and anticipated future dependence upon Austrianova and others for the manufacture of our product candidates may adversely affect our future profit margins and our ability to commercialize any products that receive marketing approval on a timely and competitive basis.
Disruptions in the global economy and supply chains may have a material adverse effect on our business, financial condition and results of operations and the financial condition of the third parties on which we rely, including Austrianova.
The disruptions to the global economy in 2020, 2021 and into 2022 have impeded global supply chains, resulting in longer lead times and also increased critical component costs and freight expenses. Austrianova, a third-party supplier on whom we rely, from time to time has experienced significant supply chain disruptions, some of which may be related to COVID-19, and we believe it may be experiencing liquidity issues. Despite any actions we have undertaken to minimize the impacts from disruptions to the global economy, there can be no assurances that unforeseen future events in the global supply chain, inflationary pressures, and delays our third parties face will not have a material adverse effect on our business, financial condition and results of operations.
Our business could be impacted as a result of actions by activist shareholders, including as a result of a potential proxy contest for the election of directors at our annual meeting.
We recently received notice from Iroquois Capital Management, LLC and certain of its affiliates nominating a slate of eight individuals for election to our Board of Directors for the 2022 annual meeting. If a proxy contest or consent solicitation results from this notice, our business could be adversely affected because: (i) responding to proxy contests and other actions by activist shareholders can be costly and time-consuming, which could disrupt our operations and divert the attention of management and our employees; (ii) perceived uncertainties as to our future direction could adversely affect our relationships with customers, suppliers, investors, prospective and current team members and others, resulting in the loss of potential business opportunities, or making it more difficult to attract and retain qualified personnel; and (iii) if individuals are elected to our board of directors with a specific agenda, it may adversely affect our ability to effectively and timely implement our strategic plan. These actions could also cause our stock price to experience periods of volatility. In addition, future proxy contests and other actions by activist shareholders could require us to incur significant legal fees and solicitation expenses and require significant time and attention by management and the Board of Directors and could materially and adversely affect our business and operating results. We may also be subject, from time to time, to other legal and business challenges in the operation of our company due to actions instituted by activist shareholders. Responding to such actions could be costly and time-consuming.
| 48 |
The recent and ongoing COVID-19 pandemic could materially affect our operations, as well as the business or operations of third parties with whom we conduct business. Our business could be adversely affected by the effects of other future health pandemics in regions where we or third parties on which we rely have significant business operations.
Our business and its operations, including, but not limited to, our proposed clinical development program, supply chain operations, research and development activities and fundraising activities, has been and could continue to be adversely affected by the COVID-19 pandemic in areas where we have business operations, including the U.S., India, Europe, Singapore and Thailand. Also, this pandemic could cause significant disruption in the operations of third parties upon whom we rely on to conduct the Company’s business. In March 2020, the World Health Organization declared the COVID-19 outbreak a pandemic. Shortly thereafter, the U.S. government-imposed restrictions on travel between the U.S., Europe, and certain other countries. The President of the U.S. declared the COVID-19 pandemic a national emergency. Since March 2020, numerous state, regional and local jurisdictions, including the jurisdictions where our headquarters are located, as well as foreign jurisdictions, have imposed, and others in the future may impose, quarantines, shelter-in-place orders, executive, and similar government orders for their residents to control the spread of COVID-19. The COVID-19 pandemic has had an impact upon our operations.
The effects of the executive orders, the shelter-in-place orders and our work-from-home policies has and may continue to negatively impact productivity, disrupt our business, and delay our proposed clinical development program and timeline, the magnitude of which will depend, in part, on the length and severity of the restrictions and other limitations on our ability to conduct our business in the ordinary course. These and similar, and perhaps more severe, disruptions in our operations could negatively impact our business, operating results and financial condition.
Quarantines, shelter-in-place, executive, and similar government orders, or the perception that such orders, shutdowns or other restrictions on the conduct of business operations could occur, related to COVID-19, could impact personnel at our third-party manufacturing facilities in Thailand, or the availability or cost of materials we use or require to conduct our business, including product development, which would disrupt our supply chain. Some of our suppliers and vendors of certain materials used in our operations and research and development activities are located in areas that are subject to executive orders and shelter-in-place orders. While many of these materials may be obtained from more than one supplier, port closures and other restrictions resulting from the COVID-19 pandemic may disrupt our supply chain or limit our ability to obtain sufficient materials to operate our business. To date, we are aware of certain suppliers for our research and development activities that have experienced operational delays related to the COVID-19 pandemic.
Depending upon the length of COVID-19 and whether the FDA lifts the clinical hold on our IND, we anticipate our planned clinical trial in LAPC may be affected by COVID-19. If COVID-19 continues to spread in the U.S. and elsewhere, we may experience additional disruptions that could adversely impact our business and proposed clinical trial, including: (i) delays or difficulties in enrolling patients in our Phase 2b clinical trial if the FDA allows us to go forward with such trial; (ii) delays or difficulties in clinical site activation, including difficulties in recruiting clinical site investigators and clinical site personnel; (iii) delays in clinical sites receiving the supplies and materials needed to conduct our clinical trial, including interruption in global shipping that may affect the transport of our clinical trial product; (iv) changes in local regulations as part of a response to COVID-19 which may require us to change the ways in which our clinical trial is to be conducted, which may result in unexpected costs, or to discontinue the clinical trial altogether, if allowed to proceed; (v) diversion of healthcare resources away from the conduct of clinical trials, including the diversion of hospitals serving as our clinical trial sites and hospital staff supporting the conduct of our clinical trial; (vi) interruption of key clinical trial activities, such as clinical trial site monitoring, due to limitations on travel imposed or recommended by federal or state governments, employers and others, or interruption of clinical trial subject visits and study procedures, the occurrence of which could affect the integrity of clinical trial data; (vii) risk that participants enrolled in our proposed clinical trials will acquire COVID-19 while the clinical trial is ongoing, which could impact the results of the clinical trial, including by increasing the number of observed adverse events; (viii) delays in necessary interactions with local regulators, ethics committees, and other important agencies and contractors due to limitations in employee resources or forced furlough of government employees; (ix) limitations in employee resources that would otherwise be focused on the conduct of our clinical trial because of sickness of employees or their families or the desire of employees to avoid contact with large groups of people; (x) refusal of the FDA to accept data from clinical trials in affected geographies; and (xi) interruption or delays to our clinical trial activities.
| 49 |
The spread of COVID-19, which has caused a widespread impact throughout the world, may materially affect us economically. The potential economic impact brought about COVID-19, and the duration of such impact, is difficult to assess or predict. The pandemic has resulted in significant disruption of global financial markets, which could reduce our ability to access capital and negatively affect our future liquidity. Also, a recession or market correction resulting from the spread of COVID-19 and related government orders and restrictions could materially affect our business and the value of our common stock. COVID-19 continues to evolve. The ultimate impact of COVID-19 and the mitigation efforts to address it is highly uncertain and subject to change. We do not yet know the full extent of potential delays or impacts on our business, our proposed clinical trial, healthcare systems or the global economy.
If we are unable to successfully raise additional capital, our future clinical trials and product development could be limited, and our long-term viability may be threatened.
We have experienced negative operating cash flows since our inception and have funded our operations primarily through sales of our equity securities. We may need to seek additional funds in the future through equity or debt financings, or strategic alliances with third parties, either alone or in combination with equity financings to complete our product development initiatives. These financings could result in substantial dilution to the holders of our common stock or require contractual or other restrictions on our operations or on alternatives that may be available to us. If we raise additional funds by issuing debt securities, these debt securities could impose significant restrictions on our operations. Any such required financing may not be available in amounts or on terms acceptable to us, and the failure to procure such required financing could have a material and adverse effect on our business, financial condition and results of operations, or threaten our ability to continue as a going concern.
Our operating and capital requirements during this fiscal year and thereafter will vary based on several factors, including whether we can complete the studies requested by the FDA with respect to our IND filing, whether the FDA allows us to commence our planned clinical trial for LAPC, how quickly enrollment of patients in our such trial can be commenced, the duration of the clinical trial and any change in the clinical development plans for our product candidates and the outcome, timing and cost of meeting regulatory requirements established by the FDA and the EMA or other comparable foreign regulatory authorities.
Our present and future capital requirements will be significant and will depend on many factors, including:
| · | our ability to complete the studies requested by the FDA with respect to our IND filing; | |
| · | whether the FDA lifts the clinical hold on our IND filing for LAPC; |
| · | the progress and results of our development efforts for our product candidates; |
| · | the costs, timing and outcome of regulatory review of our product candidates; |
| · | the costs and timing of preparing, filing and prosecuting patent applications, maintaining and enforcing our intellectual property rights and defending any intellectual property-related claims; |
| · | the effect of competing technological and market developments; |
| · | market acceptance of our product candidates; |
| · | the rate of progress in establishing coverage and reimbursement arrangements with domestic and international commercial third-party payors and government payors; |
| · | the extent to which we acquire or in-license other products and technologies; and |
| · | legal, accounting, insurance and other professional and business-related costs. |
| 50 |
We may not be able to acquire additional funds on acceptable terms, or at all. If we are unable to raise adequate funds, we may have to liquidate some or all of our assets, or delay or reduce the scope of or eliminate some or all of our development programs. Further, if we do not have, or are not able to obtain, sufficient funds, we may be required to delay planned and future clinical trials, including the pig study, and development or commercialization of our product candidates. We also may have to reduce the resources devoted to our product candidates or cease operations. Any of these factors could harm our operating results.
Due to the significant resources required for the development of our programs, and depending on our ability to access capital, we must prioritize development of certain product candidates. We may expend our limited resources on programs that do not yield a successful product candidate and fail to capitalize on product candidates or indications that may be more profitable or for which there is a greater likelihood of success.
We seek to maintain a process of prioritization and resource allocation to maintain an optimal balance between aggressively advancing lead programs and ensuring replenishment of our portfolio. Until such time, if ever, as the FDA lifts its clinical hold on our IND related to our planned Phase 2b clinical trial in LAPC, our Cell-in-a-Box® encapsulation technology is validated in our planned Phase 2b clinical trial, and sufficient additional funding is available, we have halted spending on behalf of our development program with respect to cannabinoids.
Due to the significant resources required for the development of our programs, we must focus our programs on specific diseases and decide which product candidates to pursue and advance and the amount of resources to allocate to each. Our decisions concerning the allocation of research, development, collaboration, management and financial resources toward particular product candidates or therapeutic areas may not lead to the development of any viable commercial product and may divert resources away from better opportunities. Similarly, our potential decisions to delay, terminate or collaborate with third parties in respect of certain programs may subsequently also prove to be suboptimal and could cause us to miss valuable opportunities. We may fail to capitalize on viable commercial products or profitable market opportunities, be required to forego or delay pursuit of opportunities with other product candidates or other diseases that may later prove to have greater commercial potential than those we choose to pursue, or relinquish valuable rights to such product candidates through collaboration, licensing or other royalty arrangements in cases in which it would have been advantageous for us to invest additional resources to retain sole development and commercialization rights. If we make incorrect determinations regarding the viability or market potential of any or all of our programs or product candidates or misread trends in the biotechnology industry, our business, prospects, financial condition and results of operations could be materially adversely affected.
We currently have no commercial revenue and may never become profitable.
Even if we can successfully achieve regulatory approval for our product candidates, we do not know what the reimbursement status of our product candidates will be or when any of these products will generate revenue for us, if at all. We have not generated, and do not expect to generate, any product revenue for the foreseeable future. We expect to continue to incur significant operating losses for the foreseeable future due to the cost of our research and development, preclinical studies and clinical trials and the regulatory approval process for our product candidates. The amount of future losses is uncertain and will depend, in part, on the rate of growth of our expenses.
Our ability to generate revenue from our product candidates also depends on numerous additional factors, including our ability to:
| · | successfully complete development activities, including the remaining preclinical studies and planned clinical trials for our product candidates; | |
| · | complete and submit NDAs or BLAs to the FDA and MAAs to the EMA, and obtain regulatory approval for indications for which there is a commercial market; | |
| · | complete and submit applications to, and obtain regulatory approval from, other foreign regulatory authorities; | |
| · | manufacture any approved products in commercial quantities and on commercially reasonable terms; | |
| · | develop a commercial organization, or find suitable partners, to market, sell and distribute approved products in the markets in which we have retained commercialization rights; | |
| · | achieve acceptance among patients, clinicians and advocacy groups for any products we develop; | |
| · | obtain coverage and adequate reimbursement from third parties, including government payors; and | |
| · | set a commercially viable price for any products for which we may receive approval. |
| 51 |
We are unable to predict the timing or amount of increased expenses, or when or if we will be able to achieve or maintain profitability. Even if we can complete the processes described above, we anticipate incurring significant costs associated with commercializing our product candidates.
To date, we have generated no revenue. Our ability to generate revenue and become profitable depends upon our ability to obtain regulatory approval for, and successfully commercialize, our product candidates that we may develop, in-license or acquire in the future.
We face substantial competition, which may result in others discovering, developing or commercializing competing products before or more successfully than we do.
The development and commercialization of new drug products is highly competitive. We face competition with respect to our current product candidates. We will face competition with respect to any product candidates that we may seek to develop or commercialize in the future. Such competition may arise from major pharmaceutical companies, specialty pharmaceutical companies and biotechnology companies worldwide. There are several large pharmaceutical and biotechnology companies that currently market products or are pursuing the development of products for the treatment of the disease indications for which we are developing our product candidates. Some of these competitive products and therapies are based on scientific approaches that are entirely different from our approach. Potential competitors also include academic institutions, government agencies and other public and private research organizations that conduct research, seek patent protection and establish collaborative arrangements for research, development, manufacturing and commercialization.
Specifically, there are numerous companies developing or marketing therapies for cancer, diabetes and malignant ascites, including many major pharmaceutical and biotechnology companies. Our commercial opportunity could be reduced or eliminated if our competitors develop and commercialize products that are safer, more effective, have fewer or less severe side effects, are more convenient or are less expensive than any products that we may develop. Our competitors also may obtain regulatory approval for their products more rapidly than we may obtain approval for ours, which could result in our competitors establishing a strong market position before we can enter the market.
Many of the companies against which we are competing or against which we may compete in the future have significantly greater financial resources and expertise in research and development, manufacturing, preclinical testing, conducting clinical trials, obtaining regulatory approvals and marketing approved products than we do. Mergers and acquisitions in the pharmaceutical and biotechnology sectors may result in even more resources being concentrated among a smaller number of our competitors. Smaller and other early-stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies. These third parties compete with us in recruiting and retaining qualified scientific and management personnel, establishing clinical trial sites and patient registration for clinical trials, as well as in acquiring technologies complementary to, or necessary for, our programs.
Our future revenues are unpredictable which causes potential fluctuations in operating results.
Because of our limited operating history as a biotech company; we are currently unable to accurately forecast our revenues. Future expense levels will likely be based largely on our marketing and development plans and estimates of future revenue. Any sales or operating results will likely generally depend on volume and timing of orders, which may not occur and on our ability to fulfill such orders, which we may not be able to do. We may be unable to adjust spending in a timely manner to compensate for any unexpected revenue shortfall. Accordingly, any significant shortfall in revenues in relation to planned expenditures could have an immediate adverse effect on our business, prospects, financial condition and results of operations. Further, as a strategic response to changes in the competitive environment, we may from time to time make certain pricing, service or marketing decisions that could have a material adverse effect on our business, prospects, financial condition and results of operations.
We may experience significant fluctuations in future operating results due to a variety of factors, many of which are outside of our control. Factors that may affect operating results include: (i) the ability to obtain and retain customers; (ii) our ability to attract new customers at a steady rate and maintain customer satisfaction with products; (iii) our announcement or introduction of new products by us or our competitors; (iv) price competition; (v) the level of use and consumer acceptance of its products; (vi) the amount and timing of operating costs and capital expenditures relating to expansion of the business, operations and infrastructure; (vii) governmental regulations; (viii) general economic conditions; (ix) delays or disruptions in our supply chain; and (x) the adverse impacts caused by COVID-19 discussed in more detail below.
| 52 |
Additional Risks Related to Regulatory Matters
If we are unable to obtain, or if there are delays in obtaining, required approval from the applicable regulatory agencies, we will not be able to commercialize our product candidates and our ability to generate revenue will be materially impaired.
Our product candidates must obtain marketing approval from the FDA for commercialization in the U.S. and from foreign regulatory agencies for commercialization in countries outside the U.S. The process of obtaining marketing approvals in the countries in which we intend to sell and distribute our product candidates is expensive and can take many years if approval is obtained at all. This process can vary substantially based upon a variety of factors, including the type, complexity and novelty of the product candidates involved. Failure to obtain marketing approval for a product candidate will prevent us from commercializing that product candidate. To date, we have not received approval to market any of our product candidates from regulatory agencies in any jurisdiction. We have no experience in filing and supporting the applications necessary to gain marketing approvals and expect to rely on third-party contract research organizations to assist us in this process. Securing marketing approval requires the submission of extensive preclinical and clinical data and supporting information to the regulatory agencies for each product candidate to establish the product candidate’s safety and efficacy. Securing marketing approval also requires the submission of information about the product manufacturing process to, and inspection of manufacturing facilities by, the regulatory agencies.
Our product candidates may not be effective, may be only moderately effective or may prove to have undesirable or unintended side effects, toxicities or other characteristics that may preclude our obtaining marketing approval or prevent or limit commercial use. Regulatory agencies have substantial discretion in the approval process and may refuse to accept any application or may decide that our data are insufficient for approval and require additional preclinical, clinical or other studies. In addition, varying interpretations of the data obtained from preclinical and clinical testing could delay, limit or prevent marketing approval of a product candidate. Changes in marketing approval policies during the development period, changes in or the enactment of additional statutes or regulations, or changes in regulatory review for each submitted product application, may also cause delays in or prevent the approval of an application. New cancer drugs frequently are indicated only for patient populations that have not responded to an existing therapy or have relapsed after such therapies. If we experience delays in obtaining approval or if we fail to obtain approval of our product candidates, the commercial prospects for our product candidates may be harmed and our ability to generate revenues will be materially impaired.
If allowed to proceed with our clinical development programs, we intend to conduct clinical trials for certain of our product candidates at sites outside of the U.S., and the U.S. regulatory agencies may not accept data from trials conducted in such locations.
Although the FDA may accept data from clinical trials conducted outside the U.S., acceptance of this data is subject to certain conditions imposed by the regulatory agencies outside of the U.S. For example, the clinical trial must be well designed and conducted and performed by qualified investigators in accordance with ethical principles. The trial population must also adequately represent the population in the country in which the clinical trial is being conducted. The data must be applicable to the U.S. population and medical practice in the U.S. in ways that the FDA deems clinically meaningful. Generally, the patient population for any clinical trial conducted outside of the U.S. must be representative of the population for whom we intend to seek approval in the U.S.
In addition, while these clinical trials are subject to the applicable local laws, the FDA acceptance of the data will be dependent upon its determination that the trials also complied with all applicable U.S. laws and regulations. There can be no assurance that the FDA will accept data from trials conducted outside of the U.S. If the FDA does not accept the data from any of our clinical trials that we determine to conduct outside the U.S., it would likely result in the need for additional trials that would be costly and time-consuming and delay or permanently halt the development of our product candidate.
In addition, the conduct of clinical trials outside the U.S. could have a significant impact on us. Risks inherent in conducting international clinical trials include:
| · | Foreign regulatory requirements that could restrict or limit our ability to conduct our clinical trials; |
| · | Administrative burdens of conducting clinical trials under multiple foreign regulatory schemes; |
| · | Foreign exchange fluctuations; and |
| · | Diminished protection of intellectual property in some countries. |
| 53 |
Our plan to first pursue a Phase 2b clinical trial before a pivotal Phase 3 trial will likely result in additional costs to us and resultant delays in the FDA review process and any future commercialization and marketing if regulatory approval is obtained.
If the FDA allows us to begin a clinical trial by lifting its clinical hold on our IND, we have determined that the data contained in previous clinical trial reports using the Cell-in-a-Box® and its Associated Technologies are not enough to advance the program to a Phase 3 pivotal trial. Therefore, we are designing a Phase 2b clinical trial that, if successful, we believe will provide the information necessary to plan a Phase 3 pivotal trial. Our determination to first conduct a Phase 2b clinical trial before conducting a pivotal Phase 3 clinical trial will likely result in additional costs to us and resultant delays in the regulatory review process and any future commercialization and marketing if regulatory approval is obtained. The same is true to a greater extent if the FDA requires us to commence a Phase 1 or other Phase 2 clinical trial instead of the planned Phase 2b clinical trial currently under clinical hold.
If we are unable to obtain, or if there are delays in obtaining, required approval from the regulatory agencies, we will not be able to commercialize our product candidates and our ability to generate revenue will be materially impaired.
Our product candidates must obtain marketing approval from the FDA for commercialization in the U.S. and from foreign regulatory agencies for commercialization in countries outside the U.S. The process of obtaining marketing approvals in the countries in which we intend to sell and distribute our product candidates is expensive and can take several years if approval is obtained at all. This process can vary substantially based upon a variety of factors, including the type, complexity and novelty of the product candidates involved. Failure to obtain marketing approval for a product candidate will prevent us from commercializing that product candidate. To date, we have not received approval to market any of our product candidates from regulatory agencies in any jurisdiction. We have no experience in filing and supporting the applications necessary to gain marketing approvals and expect to rely on third-party contract research organizations to assist us in this process. Securing marketing approval requires the submission of extensive preclinical and clinical data and supporting information to the regulatory agencies for each product candidate to establish the product candidate’s safety and efficacy. Securing marketing approval also requires the submission of information about the product manufacturing process to, and inspection of manufacturing facilities by, the regulatory agencies.
Our product candidates may not be effective, may be only moderately effective or may prove to have undesirable or unintended side effects, toxicities or other characteristics that may preclude our obtaining marketing approval or prevent or limit commercial use. Regulatory agencies have substantial discretion in the approval process and may refuse to accept any application or may decide that our data are insufficient for approval and require additional preclinical, clinical or other studies. In addition, varying interpretations of the data obtained from preclinical and clinical testing could delay, limit or prevent marketing approval of a product candidate. Changes in marketing approval policies during the development period, changes in or the enactment of additional statutes or regulations, or changes in regulatory review for each submitted product application, may also cause delays in or prevent the approval of an application. New cancer drugs frequently are indicated only for patient populations that have not responded to an existing therapy or have relapsed after such therapies. If we experience delays in obtaining approval or if we fail to obtain approval of our product candidates, the commercial prospects for our product candidates may be harmed and our ability to generate revenues will be materially impaired.
| 54 |
Development of a biologic involves a lengthy and expensive process with an uncertain outcome. We may incur additional costs or experience delays in completing or be unable to complete the development and commercialization of our product candidates.
Our Cell-in-a-Box® and ifosfamide combination product candidate has not begun clinical development, and, like others’ candidates in a similar phase of development, the risk of failure is high. It is impossible to predict when or if this product candidate or any other product candidate will prove effective or safe in humans or will receive regulatory approval. Before obtaining marketing approval from regulatory agencies for the sale of any product candidate, if allowed to proceed, we must complete preclinical development and then conduct extensive clinical trials to demonstrate the safety and efficacy of our product candidates in humans. Clinical trials are expensive, difficult to design and implement, can take several years to complete and are uncertain as to their outcome. A failure of one or more clinical trials can occur at any stage of a clinical trial. The clinical development of our product candidates is susceptible to the risk of failure inherent at any stage of drug development, including failure to demonstrate efficacy in a clinical trial or across a broad population of patients, the occurrence of severe or medically or commercially unacceptable adverse events, failure to comply with protocols or applicable regulatory requirements or determination by the regulatory agencies that a drug or biologic product is not approvable. It is possible that even if one or more of our product candidates has a beneficial effect, that effect will not be detected during clinical evaluation because of one or more of a variety of factors, including the size, duration, design, measurements, conduct or analysis of our clinical trials. Conversely, because of the same factors, our clinical trials if allowed to proceed, may indicate an apparent positive effect of a product candidate that is greater than the actual positive effect, if any. Similarly, in our clinical trials if allowed to proceed, we may fail to detect toxicity of, or intolerability caused by, our product candidates, or mistakenly believe that our product candidates are toxic or not well tolerated when that is not, in fact, the case.
The outcome of preclinical studies and early and mid-phase clinical trials may not be predictive of the success of later clinical trials, and interim results of a clinical trial do not necessarily predict overall results. Many companies in the pharmaceutical and biotechnology sectors have suffered significant setbacks in late-stage clinical trials after achieving positive results in earlier stages of development, and we cannot be certain that we will not face similar setbacks.
The design of a clinical trial can determine whether its results will support approval of a product; however, flaws in the design of a clinical trial may not become apparent until the clinical trial is well advanced or completed. We have limited experience in designing clinical trials and may be unable to design and execute a clinical trial to support marketing approval. In addition, preclinical and clinical data are often susceptible to varying interpretations and analyses. Many companies that believed their product candidates performed satisfactorily in preclinical studies and clinical trials have nonetheless failed to obtain marketing approval for their product candidates. Even if we believe that the results of clinical trials for our product candidates warrant marketing approval, the regulatory agencies may disagree and may not grant marketing approval of our product candidates or may require that we conduct initial clinical studies; the latter would require that we incur significantly increased costs and would significantly extend the clinical development timeline for our product candidates.
In some instances, there can be significant variability in safety or efficacy results between different clinical trials of the same product candidate due to numerous factors, including changes in trial procedures set forth in protocols, differences in the size and type of the patient populations, changes in and adherence to the clinical trial protocols and the rate of dropout among clinical trial participants. Any Phase 1, Phase 2 or Phase 3 clinical trial we may conduct may not demonstrate the efficacy and safety necessary to obtain regulatory approval to market our product candidates.
We are seeking FDA approval to commence clinical trials in the U.S. of certain of our product candidates based on clinical data that was obtained in trials conducted outside the U.S., and it is possible that the FDA may not accept data from trials conducted in such locations or conducted nearly 20 years ago.
In support of our IND application to commence a Phase 2b clinical trial in LAPC using genetically -engineered live human cells encapsulated using our Cell-in-a-Box® technology in combination with ifosfamide we are relying on a Phase 1/2 clinical trial and a Phase 2 clinical trial previously conducted using the same technology in combination with ifosfamide between 1998 and 1999 and between 1999 and 2000, respectively. The Phase 1/2 clinical trial was carried out at the Division of Gastroenterology, University of Rostock, Germany, and the Phase 2 clinical trial was carried out at four centers in two countries in Europe: Berne, Switzerland, and in Rostock, Munich and Berlin, Germany.
| 55 |
Although the FDA may accept data from clinical trials conducted outside the U.S., acceptance of this data is subject to certain conditions imposed by the FDA. There is a risk that the FDA may not accept the data from the two previous trials. In that case, we may be required to conduct a Phase 1 or a Phase 1/2b clinical trial rather than the planned Phase 2b clinical trial in LAPC, currently under clinical hold. This may result in additional costs to us and resultant delays in the regulatory review process and any future commercialization and marketing if regulatory approval is obtained. It is not known whether the FDA would be likely to reject the use of such clinical data due to the significant time that has elapsed since the earlier clinical trials were conducted or because the clinical trial material for our proposed Phase 2b clinical trial is different from that used in the earlier clinical trials because of cloning the cells used in the earlier trials and certain other modifications and improvements that have been made to the Cell-in-a-Box® technology since the time of the earlier trials.
We intend to conduct clinical trials for certain of our product candidates at sites outside of the U.S., and the U.S. regulatory agencies may not accept data from trials conducted in such locations.
Although the FDA may accept data from clinical trials conducted outside the U.S., acceptance of this data is subject to certain conditions imposed by the regulatory agencies outside of the U.S. For example, the clinical trial must be well designed and conducted and performed by qualified investigators in accordance with ethical principles. The trial population must also adequately represent the population in the country in which the clinical trial is being conducted. The data must be applicable to the U.S. population and medical practice in the U.S. in ways that the FDA deems clinically meaningful. Generally, the patient population for any clinical trial conducted outside of the U.S. must be representative of the population for whom we intend to seek approval in the U.S.
In addition, while these clinical trials are subject to the applicable local laws, the FDA acceptance of the data will be dependent upon its determination that the trials also complied with all applicable U.S. laws and regulations. There can be no assurance that the FDA will accept data from trials conducted outside of the U.S. If the FDA does not accept the data from any of our clinical trials that we determine to conduct outside the U.S., it would likely result in the need for additional trials that would be costly and time-consuming and delay or permanently halt the development of our product candidate.
In addition, the conduct of clinical trials outside the U.S. could have a significant impact on us. Risks inherent in conducting international clinical trials include:
| · | Foreign regulatory requirements that could restrict or limit our ability to conduct our clinical trials; | |
| · | Administrative burdens of conducting clinical trials under multiple foreign regulatory schemes; | |
| · | Foreign exchange fluctuations; and | |
| · | Diminished protection of intellectual property in some countries. |
If clinical trials of our product candidates fail to demonstrate safety and efficacy to the satisfaction of the regulatory agencies, we may incur additional costs or experience delays in completing or be unable to complete the development and commercialization of these product candidates.
We are not permitted to commercialize, market, promote or sell any product candidate in the U.S. without obtaining marketing approval from the FDA. Comparable regulatory agencies outside of the U.S., such as the EMA in the European Union, impose similar restrictions. We may never receive such approvals. We may be required to complete additional preclinical development and clinical trials to demonstrate the safety and efficacy of our product candidates in humans before we will be able to obtain these approvals.
Clinical testing is expensive, difficult to design and implement, can take many years to complete and is inherently uncertain as to outcome. We have not previously submitted an NDA, a BLA or a MAA to regulatory agencies for any of our product candidates.
| 56 |
Any inability to successfully complete preclinical and clinical development could result in additional costs to us and impair our ability to generate revenues from product sales, regulatory and commercialization milestones and royalties. In addition, if: (i) we are required to conduct additional clinical trials or other testing of our product candidates beyond the trials and testing that we contemplate; (ii) we are unable to successfully complete our planned clinical trials of our product candidates or other testing; (iii) the results of these trials or tests are unfavorable, uncertain or are only modestly favorable; or (iv) there are unacceptable safety concerns associated with our product candidates, we, in addition to incurring additional costs, may:
| · | Be delayed in obtaining marketing approval for our product candidates; |
| · | Not obtain marketing approval at all; |
| · | Obtain approval for indications or patient populations that are not as broad as we intended or desired; |
| · | Obtain approval with labeling that includes significant use or distribution restrictions or significant safety warnings, including “black-box” warnings; |
| · | Be subject to additional post-marketing testing or other requirements; or |
| · | Be required to remove the product from the market after obtaining marketing approval. |
Results in previous clinical trials of our encapsulated live cell and ifosfamide combination for pancreatic cancer may not be replicated in future clinical trials which could result in development delays or a failure to obtain marketing approval.
Results in the previous Phase 1/2 and Phase 2 clinical trials of the encapsulated live cell and ifosfamide combination product may not be predictive of similar results in future clinical trials such as our planned Phase 2b clinical trial in LAPC, if allowed to proceed. The previous Phase 1/2 and Phase 2 clinical trials had a relatively limited number of patients in each trial. These trials resulted in outcomes that were not statistically significant and may not be representative of future results. In addition, interim results obtained after a clinical trial has commenced do not necessarily predict results in future clinical trials. Numerous companies in the pharmaceutical and biotechnology industries have suffered significant setbacks in late-stage clinical trials even after achieving promising results in early-stage clinical development. Our clinical trials, if allowed to proceed, may produce negative or inconclusive results and we may decide, or regulatory agencies may require us, to conduct additional clinical trials. Moreover, clinical data are often susceptible to varying interpretations and analyses, and many companies that believed their product candidates performed satisfactorily in preclinical studies and clinical trials have nonetheless failed to obtain the approval for their products by the regulatory agencies.
If we experience any unforeseen events in the clinical trials of our product candidates, potential marketing approval or commercialization of our product candidates could be delayed or prevented.
We may experience numerous unforeseen events during our clinical trials, if allowed to proceed, that could delay or prevent marketing approval of our product candidates, including:
| · | Clinical trials of our product candidates may produce unfavorable or inconclusive results; |
| · | We may decide, or regulators may require us, to conduct additional clinical trials or abandon product development programs or candidates; |
| · | The number of patients required for clinical trials of our product candidates may be larger than we anticipate, patient enrollment in these clinical trials may be slower than we anticipate, or participants may drop out of these clinical trials at a higher rate than we anticipate; |
| · | Our third-party contractors, including those manufacturing our product candidates, components, or ingredients thereof or conducting clinical trials on our behalf, may fail to comply with regulatory requirements or meet their contractual obligations to us in a timely manner or at all; |
| 57 |
| · | Regulators or IRBs may not authorize us or our investigators to commence a clinical trial or conduct a clinical trial at a prospective trial site; |
| · | We may experience delays in reaching or may fail to reach agreement on acceptable clinical trial contracts or clinical trial protocols with prospective trial sites; |
| · | Patients who enroll in a clinical trial may misrepresent their eligibility to do so or may otherwise not comply with the clinical trial protocol, resulting in the need to drop the patients from the clinical trial, increase the needed enrollment size for the clinical trial or extend the clinical trial’s duration; |
| · | We may have to suspend or terminate clinical trials of our product candidates for various reasons, including a finding that the participants are being exposed to unacceptable health risks, undesirable side effects or other unexpected characteristics of a product candidate; |
| · | Regulatory agencies or IRBs may require that we or our investigators suspend or terminate clinical research for various reasons, including noncompliance with regulatory requirements or their respective standards of conduct, a finding that the participants are being exposed to unacceptable health risks, undesirable side effects or other unexpected characteristics of the product candidate or findings of undesirable effects caused by a chemically or mechanistically similar drug or drug candidate; |
| · | Regulatory agencies may disagree with our clinical trial design or our interpretation of data from preclinical studies and clinical trials; |
| · | Regulatory agencies may fail to approve or subsequently find fault with the manufacturing processes or facilities of third-party manufacturers with which we enter agreements for clinical and commercial supplies; |
| · | The supply or quality of raw materials or manufactured product candidates or other materials necessary to conduct clinical trials of our product candidates may be insufficient, inadequate, delayed, or not available at an acceptable cost, or we may experience interruptions in supply; and |
| · | The approval policies or regulations of the regulatory agencies may significantly change in a manner rendering our clinical data insufficient to obtain marketing approval. |
Product development costs for us will increase if we experience delays in testing or pursuing marketing approvals. We may also be required to obtain additional funds to complete clinical trials and prepare for possible commercialization of our product candidates. We do not know whether any preclinical studies or clinical trials will begin as planned, will need to be restructured or will be completed on schedule or at all. Significant preclinical study or clinical trial delays also could shorten any periods during which we may have the exclusive right to commercialize our product candidates or allow our competitors to bring products to market before we do and impair our ability to successfully commercialize our product candidates and may harm our business and results of operations. In addition, many of the factors that cause, or lead to, clinical trial delays may ultimately lead to the denial of marketing approval of any of our product candidates.
If we experience delays or difficulties in the enrollment of patients in clinical trials, we may not achieve our clinical development timeline and our receipt of necessary regulatory approvals could be delayed or prevented.
We may not be able to initiate or continue clinical trials for our product candidates if we are unable to locate and enroll enough eligible patients to participate in our clinical trials. Patient enrollment is a significant factor in the overall duration of a clinical trial and is affected by many factors, including:
| · | The size and nature of the patient population; | |
| · | The severity of the disease under investigation; | |
| · | The proximity of patients to clinical sites; | |
| · | The eligibility criteria for the trial; | |
| · | The design of the clinical trial; | |
| · | Efforts to facilitate timely enrollment; | |
| · | Competing clinical trials for the same patient population; and | |
| · | Clinicians’ and patients’ perceptions as to the potential advantages and risks of the drug being studied in relation to other available therapies, including any new drugs that may be approved for the indications we are investigating. |
| 58 |
Our inability to enroll enough patients for our clinical trials could result in significant delays or may require us to abandon one or more clinical trials altogether. Enrollment delays in our clinical trials may result in increased development costs for our product candidates, delay or halt the development of and approval processes for our product candidates and jeopardize our ability to achieve our clinical development timeline and goals, including the dates by which we will commence, complete and receive results from clinical trials. Enrollment delays may also delay or jeopardize our ability to commence sales and generate revenues from our product candidates. Any of the foregoing could cause the value of our company to decline and limit our ability to obtain additional financing, if needed.
We may request priority review for our product candidates in the future. The regulatory agencies may not grant priority review for any of our product candidates. Moreover, even if the regulatory agencies designated such products for priority review, that designation may not lead to a faster regulatory review or approval process and, in any event, does not assure approval by the regulatory agencies.
We may be eligible for priority review designation for our product candidates if the regulatory agencies determine such product candidates offer major advances in treatment or provide a treatment where no adequate therapy exists. A priority review designation means that the time required for the regulatory agencies to review an application is less than the standard review period. The regulatory agencies have broad discretion with respect to whether to grant priority review status to a product candidate, so even if we believe a product candidate is eligible for such designation or status, the regulatory agencies may decide not to grant it. Thus, while the regulatory agencies have granted priority review to other oncology and diabetes products, our product candidates, should we determine to seek priority review of them, may not receive similar designation. Moreover, even if one of our product candidates is designated for priority review, such a designation does not necessarily mean a faster overall regulatory review process or necessarily confer any advantage with respect to approval compared to conventional procedures of the regulatory agencies.
Receiving priority review from the regulatory agencies does not guarantee approval within an accelerated timeline or thereafter.
In some instances, we believe we may be able to secure approval from the regulatory agencies to use accelerated development pathways. If we are unable to obtain such approval, we may be required to conduct additional preclinical studies or clinical trials beyond those that we contemplate which could increase the expense of obtaining and delay the receipt of necessary marketing approvals.
We anticipate that we may seek an accelerated approval pathway for certain of our product candidates. Under the accelerated approval provisions or their implementing regulations of the regulatory agencies, they may grant accelerated approval to a product designed to treat a serious or life-threatening condition that provides meaningful therapeutic benefit over available therapies upon a determination that the product influences a surrogate endpoint or intermediate clinical endpoint that is reasonably likely to predict clinical benefit. Regulatory agencies consider a clinical benefit to be a positive therapeutic effect that is clinically meaningful in the context of a given disease, such as irreversible morbidity or mortality. For the purposes of accelerated approval, a surrogate endpoint is a marker, such as a laboratory measurement, radiographic image, physical sign or other measure that is thought to predict clinical benefit but is not itself a measure of clinical benefit. An intermediate clinical endpoint is a clinical endpoint that can be measured earlier than an effect on irreversible morbidity or mortality that is reasonably likely to predict an effect on irreversible morbidity or mortality or other clinical benefit. The accelerated approval pathway may be used in cases in which the advantage of a new drug over available therapy may not be a direct therapeutic advantage but is a clinically important improvement from a patient and public health perspective. If granted, accelerated approval is usually contingent on the sponsor’s agreement to conduct, in a diligent manner, additional post-approval confirmatory studies to verify and describe the drug’s clinical benefit. If such post-approval studies fail to confirm the drug’s clinical benefit, regulatory agencies may withdraw their approval of the drug.
Prior to seeking such accelerated approval, we will seek feedback from the regulatory agencies and will otherwise evaluate our ability to seek and receive such accelerated approval. There can also be no assurance that after our evaluation of the feedback and other factors we will decide to pursue or submit an NDA, a BLA or an MAA for accelerated approval or any other form of expedited development, review or approval. Similarly, there can be no assurance that after subsequent feedback from regulatory agencies that we will continue to pursue or apply for accelerated approval or any other form of expedited development, review or approval, even if we initially decide to do so. Furthermore, if we decide to apply for accelerated approval or under another expedited regulatory designation (such as the Breakthrough Therapy designation or Fast Track designation), there can be no assurance that such submission or application will be accepted or that any expedited development, review or approval will be granted on a timely basis or at all. Regulatory agencies could also require us to conduct further studies prior to considering our application or granting approval of any type. A failure to obtain accelerated approval or any other form of expedited development, review or approval for any of our product candidates that we determine to seek accelerated approval for would result in a longer time to commercialization of such product candidate, could increase the cost of development of such product candidate and could harm our competitive position in the marketplace.
| 59 |
We may seek Orphan Drug designation for some of our product candidates, and we may be unsuccessful.
Regulatory agencies may designate drugs for relatively small patient populations as Orphan Drugs. Under the standards and requirements of regulatory agencies, they may designate a product as an Orphan Drug if it is a drug intended to treat a rare disease or condition. In the U.S., this is generally defined as a disease with a patient population of fewer than 200,000 individuals. If a product with an Orphan Drug designation subsequently receives the first marketing approval for the indication for which it has such designation, the product is entitled to a period of marketing exclusivity, which precludes the EMA or FDA from approving another marketing application for the same drug for the same indication during the period of exclusivity. The applicable period is seven years in the U.S. and ten years in Europe. In Europe, a product must meet the orphan prevalence not only when so designated but at marketing authorization. The European exclusivity period can be reduced to six years if a drug no longer meets the criteria for Orphan Drug designation or if the drug is sufficiently profitable so that market exclusivity is no longer justified.
We have been granted Orphan Drug designation for our pancreatic cancer therapy in the U.S. and European Union. Orphan Drug exclusivity may be lost if a regulatory agency determines that the request for designation was materially defective or if the manufacturer is unable to assure sufficient quantity of the drug to meet the needs of patients with the rare disease or condition. Marketing exclusivity for a product designated as an Orphan Drug may not effectively protect the product candidate from competition because different drugs can be approved for the same condition, and the same drug may be approved for a different condition that may be used offlabel for an orphan indication. Even after an Orphan Drug is approved and granted exclusivity, the regulatory agency can subsequently approve the same drug in a different drug product for the same condition if they conclude that the later drug is clinically superior in that it is shown to be safer, more effective or makes a major contribution to patient care.
A Fast Track by the FDA or similar designation by another regulatory agency, even if granted for any of our product candidates, may not lead to a faster development or regulatory review or approval process and does not increase the likelihood that our product candidates will receive marketing approval.
We do not currently have Fast Track designation by the FDA or similar designation by another regulatory agency for any of our product candidates but intend to seek such designation based upon the data generated from our clinical trials, if allowed to proceed and if successful. If a drug or biologic is intended for the treatment of a serious or life-threatening condition and the product candidate demonstrates the potential to address unmet medical needs for this condition, the sponsor may apply for Fast Track designation by the FDA or similar designation by another regulatory agency. Regulatory agencies have broad discretion whether to grant this designation by the FDA or similar designation by another regulatory agency. Even if we believe a product candidate is eligible for this designation, we cannot assure you that a regulatory agency would decide to grant it. Even if we do receive Fast Track or similar designation, we may not experience a faster development process, review or approval compared to conventional procedures adopted by a regulatory agency. In addition, a regulatory agency may withdraw Fast Track designation if it believes that the designation is no longer supported by data from our clinical development program. Many product candidates that have received Fast Track designation have failed to obtain marketing approval.
A Breakthrough Therapy designation by the FDA or similar designation by another regulatory agency, even if granted for any of our product candidates, may not lead to a faster development or regulatory review or approval process and does not increase the likelihood that our product candidates will receive marketing approval.
We do not currently have Breakthrough Therapy designation by the FDA or similar designation by another regulatory agency for any of our product candidates but intend seek such designation based upon the data we generate during our clinical trials, if successful.
A Breakthrough Therapy or similar designation is within the discretion of the FDA and other regulatory agencies. Accordingly, even if we believe, after completing early clinical trials, that one of our product candidates meets the criteria for designation as a Breakthrough Therapy or other similar designation, a regulatory agency may disagree and instead determine not to make such designation. In any event, the receipt of a Breakthrough Therapy or other similar designation for a product candidate may not result in a faster development process, review or approval compared to drugs or biologics considered for approval under conventional procedures of a regulatory agency and does not assure their ultimate approval. In addition, even if one or more of our product candidates receives Breakthrough Therapy designation or other similar designations, a regulatory agency may later decide that such product candidates no longer meet the conditions for the designation.
| 60 |
Failure to obtain marketing approval in international jurisdictions would prevent our product candidates from being marketed abroad.
To market and sell our product candidates in Europe and many other jurisdictions outside the U.S., we or our third-party collaborators must obtain separate marketing approvals and comply with numerous and varying regulatory requirements. The approval procedure varies among countries and can involve additional testing. The time required to obtain approval may differ substantially from that required to obtain FDA approval in the U.S. The regulatory approval process outside the U.S. generally includes all the risks associated with obtaining FDA approval. In addition, in many countries outside the U.S., it is required that the product be approved for reimbursement before the product can be approved for sale in that country. We or these third parties may not obtain approval from a regulatory agency outside the U.S. on a timely basis, if at all. Approval by FDA does not ensure approval by a regulatory agency in other countries or jurisdictions, and approval by one regulatory agency outside the U.S. does not ensure approval by a regulatory agency in other countries or jurisdictions or by the FDA. We may not be able to file for marketing approvals and may not receive necessary approvals to commercialize our product candidates in any market.
Any product candidate for which we obtain marketing approval will be subject to extensive post-marketing regulatory requirements and could be subject to post-marketing restrictions or withdrawal from the market. We may be subject to penalties if we fail to comply with regulatory requirements or if we experience unanticipated problems with our products, when and if any of our product candidates are approved.
Our product candidates and the activities associated with their development and commercialization, including their testing, manufacture, recordkeeping, labeling, storage, approval, advertising, promotion, sale and distribution, are subject to comprehensive regulation by regulatory agencies. The requirements that result from such regulations include submissions of safety and other post-marketing information and reports, registration and listing requirements, cGMP requirements relating to manufacturing, quality control, quality assurance and corresponding maintenance of records and documents, including periodic inspections by regulatory agencies, requirements regarding the distribution of samples to physicians and recordkeeping.
In addition, regulatory agencies may impose requirements for costly post-marketing studies or clinical trials and surveillance to monitor the safety or efficacy of a product candidate. Regulatory agencies tightly regulate the post-approval marketing and promotion of drugs and biologics to ensure the products are marketed only for the approved indications and in accordance with the provisions of the approved labeling. They also impose stringent restrictions on manufacturers’ communications regarding use of their products. If we promote our product candidates beyond their approved indications, we may be subject to enforcement action for off-label promotion. Violations of the laws relating to the promotion of prescription drugs or biologics may lead to investigations alleging violations of federal and state healthcare fraud and abuse laws, as well as state consumer protection laws.
Also, later discovery of previously unknown adverse events or other problems with our product candidates, manufacturers or manufacturing processes, or failure to comply with regulatory requirements, may yield various results, including:
| · | Restrictions on such products, manufacturers or manufacturing processes; | |
| · | Restrictions on the labeling or marketing of a product; | |
| · | Restrictions on product distribution or use; | |
| · | Requirements to conduct post-marketing studies or clinical trials; | |
| · | Warning or untitled letters or Form 483s; | |
| · | Withdrawal of the products from the market; |
| 61 |
| · | Refusal to approve pending applications or supplements to approved applications that we submit; | |
| · | Recall of products; | |
| · | Fines, restitution or disgorgement of profits or revenues; | |
| · | Suspension or withdrawal of marketing approvals; | |
| · | Refusal to permit the import or export of our product candidates; | |
| · | Product seizure; or | |
| · | Injunctions or the imposition of civil or criminal penalties |
Non-compliance with European requirements regarding safety monitoring or pharmacovigilance, and with requirements related to the development of products for the pediatric population, can also result in significant financial penalties. Similarly, failure to comply with the Europe’s requirements regarding the protection of personal information can also lead to significant penalties and sanctions.
Our relationships with customers and third-party payors will be subject to applicable anti-kickback, fraud and abuse and other healthcare laws and regulations, which could expose us to criminal sanctions, substantial civil penalties, contractual damages, reputational harm and diminished profits and future earnings.
Healthcare providers, physicians and third-party payors will play a primary role in the recommendation and prescription of any product candidates for which we obtain marketing approval. Our future arrangements with third-party payors and customers may expose us to applicable federal and state fraud and abuse and other healthcare laws and regulations that may constrain the business or financial arrangements and relationships through which we market, sell and distribute any products for which we obtain marketing approval. Restrictions under applicable healthcare laws and regulations include the following:
The Anti-Kickback Statute prohibits, among other things, persons from knowingly and willfully soliciting, offering, receiving or providing any remuneration, directly or indirectly, in cash or in kind, to induce or reward, or in return for, either the referral of an individual for, or the purchase, order or recommendation of, any good or service, for which payment may be made under a federal healthcare program such as Medicare and Medicaid;
The False Claims Act imposes criminal and civil penalties, including civil whistleblower or qui tam actions, against individuals or entities for knowingly presenting, or causing to be presented, to the federal government, claims for payment that are false or fraudulent or making a false statement to avoid, decrease or conceal an obligation to pay money to the Federal governments; and
HIPAA imposes criminal and civil liability for executing a scheme to defraud any healthcare benefit program or making false statements relating to healthcare matters. HIPAA, as amended by HITECH and its implementing regulations, also imposes obligations, including mandatory contractual terms, with respect to safeguarding the privacy, security and transmission of individually identifiable health information. Federal law requires applicable manufacturers of covered drugs to report payments and other transfers of value to physicians and teaching hospitals, which includes data collection and reporting obligations. The information is to be made publicly available on a searchable website. Analogous state and foreign laws and regulations, such as state anti-kickback and false claims laws, may apply to sales or marketing arrangements and claims involving healthcare items or services reimbursed by non-governmental third-party payors, including private insurers.
Some state laws require pharmaceutical companies to comply with the pharmaceutical industry’s voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government and may require drug manufacturers to report information related to payments and other transfers of value to physicians and other healthcare providers or marketing expenditures. State and foreign laws also govern the privacy and security of health information in some circumstances, many of which differ from each other in significant ways and often are not preempted by HIPAA, thus complicating compliance efforts.
| 62 |
Efforts to ensure that our business arrangements with third parties will comply with applicable healthcare laws and regulations will involve substantial costs. It is possible that governmental authorities will conclude that our business practices may not comply with current or future statutes, regulations or case law involving applicable fraud and abuse or other healthcare laws and regulations. If our operations are found to be in violation of any of these laws or any other governmental regulations that may apply to us, we may be subject to significant civil, criminal and administrative penalties, damages, fines, imprisonment, exclusion of our product candidates from government funded healthcare programs, such as Medicare and Medicaid, and the curtailment or restructuring of our operations. If any of the physicians or other healthcare providers or entities with whom we expect to do business is found to be not in compliance with applicable laws, they may be subject to criminal, civil or administrative sanctions, including exclusions from government funded healthcare programs.
Recently enacted and future legislation could increase the difficulty and cost for us to obtain marketing approval of and commercialize our product candidates and affect the prices we may obtain.
The United States and many foreign jurisdictions have enacted or proposed legislative and regulatory changes affecting the healthcare system that may affect our ability to profitably sell our product candidates, if approved. The United States government, state legislatures and foreign governments also have shown significant interest in implementing cost-containment programs to limit the growth of government-paid healthcare costs, including price controls, restrictions on reimbursement and requirements for substitution of generic products for branded prescription drugs and biologics.
The Affordable Care Act was intended to broaden access to health insurance, reduce or constrain the growth of healthcare spending, enhance remedies against fraud and abuse, add transparency requirements for the healthcare and health insurance industries, impose new taxes and fees on the health industry and impose additional health policy reforms.
We expect that the Affordable Care Act, as well as other healthcare reform measures that have and may be adopted in the future, may result in more rigorous coverage criteria and in additional downward pressure on the price that we receive for our product candidates, if approved, and could seriously harm our future revenues. Any reduction in reimbursement from Medicare, Medicaid, or other government programs may result in a similar reduction in payments from private payers. The implementation of cost containment measures or other healthcare reforms may prevent us from being able to generate revenue, attain and maintain profitability of our product candidates, if approved.
Governments outside the U.S. tend to impose strict price controls, which may adversely affect our revenues, if any.
In some countries, particularly the EEA countries and the United Kingdom, the pricing of prescription pharmaceuticals is subject to governmental control. In these countries, pricing negotiations with governmental authorities can take considerable time after the receipt of marketing approval for a product. To obtain reimbursement or pricing approval in some countries, we may be required to conduct a clinical trial that compares the cost-effectiveness of our product candidate to other available therapies. If reimbursement of our product candidates is unavailable or limited in scope or amount, or if pricing is set at unsatisfactory levels, our business could be materially harmed.
Risks Related to the Commercialization of Our Product Candidates
Serious adverse events or undesirable side effects or other unexpected properties of our encapsulated live cell plus ifosfamide product candidate or any of our other product candidates may be identified during development that could delay or prevent the product candidates’ marketing approval.
Serious adverse events or undesirable side effects caused by, or other unexpected properties of, our product candidates could cause us, an IRB or a regulatory agency to interrupt, delay or halt clinical trials of one or more of our product candidates and could result in a more restrictive label or the delay or denial of marketing approval by a regulatory agency. If any of our product candidates is associated with serious adverse events or undesirable side effects or has properties that are unexpected, we may need to abandon development or limit development of that product candidate to certain uses or subpopulations in which the undesirable side effects or other characteristics are less prevalent, less severe or more acceptable from a risk-benefit perspective. Many drugs that initially showed promise in clinical or earlier stage testing have later been found to cause undesirable or unexpected side effects that prevented further development of the drug.
| 63 |
Even if one of our product candidates receives marketing approval, it may fail to achieve the degree of market acceptance by physicians, patients, third party payors and others in the medical community necessary for commercial success and the market opportunity for the product candidate may be smaller than we anticipated.
We have never commercialized a drug or biologic product. Even if one of our product candidates is approved by a regulatory agency for marketing and sale, it may nonetheless fail to gain sufficient market acceptance by physicians, patients, third party payors and others in the medical community. For example, physicians are often reluctant to switch their patients from existing therapies even when new and potentially more effective or convenient treatments enter the market. Further, patients often acclimate to the therapy that they are currently taking and do not want to switch unless their physicians recommend switching products or they are required to switch therapies due to lack of reimbursement for existing therapies.
Efforts to educate the medical community and third-party payors on the benefits of our product candidates may require significant resources and may not be successful. If any of our product candidates is approved but does not achieve an adequate level of market acceptance, we may not generate significant revenues and we may not become profitable.
The degree of market acceptance of our encapsulated live cell plus ifosfamide product candidate or any of our other product candidates, if approved for commercial sale, will depend on several factors, including:
| · | The efficacy and safety of the product; | |
| · | The potential advantages of the product compared to alternative treatments; | |
| · | The prevalence and severity of any side effects; | |
| · | The clinical indications for which the product is approved; | |
| · | Whether the product is designated under physician treatment guidelines as a first-line therapy or as a second- or third-line therapy; | |
| · | Limitations or warnings, including distribution or use restrictions, contained in the product’s approved labeling; | |
| · | Our ability to offer the product for sale at competitive prices; | |
| · | Our ability to establish and maintain pricing sufficient to realize a meaningful return on our investment; | |
| · | The product’s convenience and ease of administration compared to alternative treatments; | |
| · | The willingness of the target patient population to try, and of physicians to prescribe, the product; | |
| · | The strength of sales, marketing and distribution support; | |
| · | The approval of other new products for the same indications; | |
| · | Changes in the standard of care for the targeted indications for the product; | |
| · | The timing of market introduction of our approved products as well as competitive products and other therapies; | |
| · | Availability and amount of reimbursement from government payors, managed care plans and other third-party payors; | |
| · | Adverse publicity about the product or favorable publicity about competitive products; and | |
| · | Potential product liability claims. |
| 64 |
The potential market opportunities for our product candidates are difficult to estimate precisely. Our estimates of the potential market opportunities are predicated on many assumptions, including industry knowledge and publications, third party research reports and other surveys. While we believe that our internal assumptions are reasonable, these assumptions involve the exercise of significant judgment on the part of our management, are inherently uncertain and the reasonableness of these assumptions has not been assessed by an independent source. If any of the assumptions proves to be inaccurate, the actual markets for our product candidates could be smaller than our estimates of the potential market opportunities.
If any of our product candidates receives marketing approval and we or others later discover that the therapy is less effective than previously believed or causes undesirable side effects that were not previously identified, our ability to market the therapy could be compromised.
Clinical trials of our product candidates, if allowed to proceed, will be conducted in carefully defined subsets of patients who have agreed to enter a clinical trial. Consequently, it is possible that our clinical trials, if allowed to proceed, may indicate an apparent positive effect of a product candidate that is greater than the actual positive effect, if any, or alternatively fail to identify undesirable side effects. If, following approval of a product candidate, we or others discover that the product candidate is less effective than previously believed or causes undesirable side effects that were not previously identified, any of the following adverse events could occur:
| · | A regulatory agency may withdraw its approval of the product candidate or seize the product candidate; | |
| · | We may be required to recall the product candidate or change the way the product is administered; | |
| · | Additional restrictions may be imposed on the marketing of, or the manufacturing processes for, the product candidate; | |
| · | We may be subject to fines, injunctions or the imposition of civil or criminal penalties; | |
| · | A regulatory agency may require the addition of labeling statements, such as a “black box” warning or a contraindication; | |
| · | We may be required to create a Medication Guide outlining the risks of the previously unidentified side effects for distribution of our product candidate to patients; | |
| · | We could be sued and held liable for harm caused to patients; | |
| · | The product candidate may become less competitive; and | |
| · | Our reputation may suffer. |
Any of these events could have a material and adverse effect on our operations and business and could adversely impact our stock price.
If we are unable to establish sales, marketing and distribution capabilities or enter acceptable sales, marketing and distribution arrangements with third parties, we may not be successful in commercializing any product candidate that we develop when a product candidate is approved.
We do not have any sales, marketing or distribution infrastructure and have no experience in the sale, marketing or distribution of pharmaceutical products. To achieve commercial success for any approved product candidate, we must either develop a sales and marketing organization, outsource these functions to third parties or license our product candidates to others. If approved by the FDA, the EMA or comparable foreign regulatory agencies, we expect to license our encapsulated live cell plus ifosfamide product candidate for pancreatic cancer to a large pharmaceutical company with greater resources and experience than us.
We may not be able to license our encapsulated live cell plus ifosfamide product candidate on reasonable terms, if at all. If other product candidates are approved for smaller or easily targeted markets, we expect to commercialize them in the U.S. directly with a small and highly focused commercialization organization. The development of sales, marketing and distribution capabilities will require substantial resources and will be time-consuming, which could delay any product candidate launch.
We expect that we will commence the development of these capabilities prior to receiving approval of any of our product candidates. If the commercial launch of a product candidate for which we recruit a sales force and establish marketing and distribution capabilities is delayed or does not occur for any reason, we could have prematurely or unnecessarily incurred these commercialization costs. Such a delay may be costly, and our investment could be lost if we cannot retain or reposition our sales and marketing personnel.
| 65 |
In addition, we may not be able to hire or retain a sales force in the U.S. that is sufficient in size or has adequate expertise in the medical markets that we plan to target. If we are unable to establish or retain a sales force and marketing and distribution capabilities, our operating results may be adversely affected. If a potential partner has development or commercialization expertise that we believe is particularly relevant to one of our product candidates, then we may seek to collaborate with that potential partner even if we believe we could otherwise develop and commercialize the product candidate independently.
We expect to seek one or more strategic partners for commercialization of our product candidates outside the U.S. Because of entering arrangements with third parties to perform sales, marketing and distribution services, our product revenues or the profitability of these product revenues may be lower, perhaps substantially lower, than if we were to directly market and sell products in those markets. Furthermore, we may be unsuccessful in entering the necessary arrangements with third parties or may be unable to do so on terms that are favorable to us. In addition, we may have little or no control over such third parties and any of them may fail to devote the necessary resources and attention to sell and market our product candidates effectively.
If we do not establish sales and marketing capabilities, either on our own or in collaboration with third parties, we will not be successful in commercializing any of our product candidates that receive marketing approval.
Risks Related to Our Dependence on Third Parties
We rely heavily on third parties to conduct our preclinical studies and plan to rely on third parties to conduct our clinical trials, assuming they are allowed to proceed, and those third parties may not perform satisfactorily, including failing to meet deadlines for the completion of such studies and trials.
We currently rely heavily on third parties to conduct our preclinical studies and plan to rely on third parties to conduct our clinical trials, assuming they are allowed to proceed, including Austrianova in which we own an equity interest. We expect to continue to rely heavily on third parties, such as a CRO, a clinical data management organization, a medical institution, a clinical investigator and others to plan for and conduct our clinical trials. Our agreements with these third parties generally allow the third party to terminate our agreement with them at any time. If we are required to enter alternative arrangements because of any such termination, the introduction of our product candidates to market could be delayed.
Our reliance on these third parties for R&D activities will reduce our control over these activities but will not relieve us of our responsibilities. For example, we design our clinical trials and will remain responsible for ensuring that each is conducted in accordance with the general investigational plan and protocol for the trial. Moreover, regulatory agencies require us to comply with current good manufacturing practices (“cGMP”) for conducting, recording and reporting the results of clinical trials to assure that data and reported results are credible and accurate and that the rights, integrity and confidentiality of trial participants are protected. Our reliance on third parties that we do not control does not relieve us of these responsibilities and requirements. We also are required to register ongoing clinical trials and post the results of completed clinical trials on a government-sponsored database of regulatory agencies within specified timeframes. Failure to do so can result in fines, adverse publicity and civil and criminal sanctions.
Furthermore, these third parties may also have relationships with other entities, some of which may be our competitors. If these third parties do not successfully carry out their contractual duties, meet expected deadlines or conduct our clinical trials in accordance with the requirements of a regulatory agency or our protocols, we will not be able to obtain, or may be delayed in obtaining, marketing approvals for our product candidates and will not be able to, or may be delayed in our efforts to, successfully commercialize our product candidates.
In addition, disruptions in the global economy and supply chains could adversely affect the financial conditions of the third parties on which we rely, resulting in delays in preclinical studies and clinical trials that could adversely affect our business, financial condition and results of operations. For instance, Austrianova from time to time has experienced significant supply chain delays, some of which may be related to COVID-19, and we believe it may be experiencing liquidity issues.
| 66 |
We rely on numerous consultants for a substantial portion of our R&D related to our product candidates. If there are delays or failures to perform their obligations, our product candidates would be adversely affected. If our collaboration with these consultants is unsuccessful or is terminated, we would need to identify new research and collaboration partners for our preclinical and clinical development. If we are unsuccessful or significantly delayed in identifying new collaboration and research partners, or unable to reach an agreement with such a partner on commercially reasonable terms, development of our product candidates will suffer, and our business would be materially harmed.
In addition, if any of these consultants change their strategic focus, or if external factors cause any one of them to divert resources from our collaboration, or if any one of them independently develops products that compete directly or indirectly with our product candidates using resources or information it acquires from our collaboration, our business and results of operations could suffer.
Future preclinical and clinical development collaborations may be important to us. If we are unable to maintain these collaborations, or if these collaborations are not successful, our business could be adversely affected.
For some of our product candidates, we may in the future determine to collaborate with pharmaceutical and biotechnology companies for development of our product candidates. We face significant competition in seeking appropriate collaborators. Our ability to reach a definitive agreement for any collaboration will depend, among other things, upon our assessment of the collaborator’s resources and expertise, the terms and conditions of the proposed collaboration and the proposed collaborator’s evaluation of several factors. If we are unable to reach agreements with suitable collaborators on a timely basis, on acceptable terms, or at all, we may have to curtail the development of a product candidate, reduce or delay its development program or one or more of our other development programs, delay our potential development schedule or increase our expenditures and undertake preclinical and clinical development activities at our own expense. If we fail to enter collaborations and do not have sufficient funds or expertise to undertake the necessary development activities, we may not be able to further develop our product candidates or continue to develop our product candidates and our business may be materially and adversely affected.
Future collaborations we may enter may involve the following risks:
| · | Collaborators may have significant discretion in determining the efforts and resources that they will apply to these collaborations; | |
| · | Collaborators may not perform their obligations as expected; | |
| · | Changes in the collaborators’ strategic focus or available funding, or external factors, such as an acquisition, may divert resources or create competing priorities; | |
| · | Collaborators may delay discovery and preclinical development, provide insufficient funding for product development of targets selected by us, stop or abandon preclinical or clinical development of a product candidate or must repeat or conduct new preclinical and clinical development of a product candidate; | |
| · | Collaborators could independently develop, or develop with third parties, products that compete directly or indirectly with our products or product candidates if the collaborators believe that competitive products are more likely to be successfully developed than ours; | |
| · | Product candidates may be viewed by our collaborators as competitive with their own product candidates or products, which may cause collaborators to cease to devote resources to the development of our product candidates; | |
| · | Disagreements with collaborators, including disagreements over proprietary rights, contract interpretation or the preferred course of development might cause delays or termination of the preclinical or clinical development or commercialization of product candidates. This might lead to additional responsibilities for us with respect to product candidates, or might result in litigation or arbitration, any of which would be time-consuming and expensive; | |
| · | Collaborators may not properly maintain or defend our intellectual property rights or intellectual property rights licensed to us or may use our proprietary information in such a way as to invite litigation that could jeopardize or invalidate our intellectual property or proprietary information or expose us to potential litigation; | |
| · | Collaborators may infringe the intellectual property rights of third parties, which may expose us to litigation and potential liability; and | |
| · | Collaborations may be terminated at the convenience of the collaborator and, if terminated, we could be required to raise additional capital to pursue further development or commercialization of our product candidates. |
In addition, subject to its contractual obligations to us, if a collaborator of ours is involved in a business combination, the collaborator might deemphasize or terminate the development of any of our product candidates. If one of our collaborators terminates its agreement with us, we may find it more difficult to attract new collaborators and our perception in the business and financial communities could be adversely affected. If we are unable to maintain our collaborations, development of our product candidates could be delayed, and we may need additional resources to develop them.
| 67 |
We rely on Prof. Günzburg and Dr. Salmons for the development of our product candidates. If they decide to terminate their relationship with us, we may not be successful in the development of our product candidates.
We rely on Prof. Walter H. Günzburg and Dr. Brian Salmons, officers of Austrianova, for the development of our product candidates. If they decide to terminate their relationship with us, we may not be successful in the development of our product candidates.
Prof. Günzburg and Dr. Salmons are involved in almost all our scientific endeavors underway and being planned by us. These endeavors include preclinical and clinical studies involving our cancer therapy for LAPC to be conducted in the U.S. and elsewhere on our behalf. They also provide professional consulting services to us through the respective consulting agreements we have entered with the consulting companies through which they provide services. The consulting agreements may be terminated for any reason at any time upon one party giving the other a written notice prior to the effective date of the termination. If that occurs, we may not be successful in the development of our product candidates which could have a material adverse effect on us.
The manufacture of our product candidates is complex, and difficulties may be encountered in production. If such difficulties are encountered or failure to meet regulatory standards occurs, our ability to provide supply of our product candidates for clinical trials, if allowed to proceed, or our products for patients, if approved, could be delayed or stopped, or we may be unable to maintain a commercially viable cost structure.
The processes involved in manufacturing our product candidates are complex, expensive, highly regulated and subject to multiple risks. Even minor deviations from normal manufacturing processes could result in reduced production yields, product defects and other supply disruptions. Further, as product candidates are developed through preclinical studies to potential future clinical trials towards approval and commercialization, it is common that various aspects of the development program, such as manufacturing methods, are altered along the way in an effort to optimize processes and results. Such changes carry the risk that they will not achieve these intended objectives, and any of these changes could cause our product candidates to perform differently and affect the results of planned clinical trials or other future clinical trials. We expect to rely on third-party manufacturers for the manufacturing of our products.
In order to conduct planned or future clinical trials of our product candidates, or supply commercial products, if approved, we will need to have them manufactured in small and large quantities. Our manufacturing partners may be unable to successfully increase the manufacturing capacity for any of our product candidates in a timely or cost-effective manner, or at all. In addition, quality issues may arise during scale-up activities. If our manufacturing partners are unable to successfully scale up the manufacture of our product candidates in sufficient quality and quantity, the development, testing and potential clinical trials of that product candidate may be delayed or become infeasible, and regulatory approval or commercial launch of any resulting product may be delayed or not obtained, which could significantly harm our business. The same risks would apply to our internal manufacturing facilities, should we in the future decide to build internal manufacturing capacity. In addition, building internal manufacturing capacity would carry significant risks in terms of being able to plan, design and execute on a complex project to build manufacturing facilities in a timely and cost-efficient manner.
In addition, the manufacturing process for any products that we may develop is subject to FDA, EMA and foreign regulatory authority approval processes and continuous oversight, and we will need to contract with manufacturers who can meet all applicable FDA, EMA and foreign regulatory authority requirements, including complying with current good manufacturing processes, or on an ongoing basis. If we or our third-party manufacturers are unable to reliably produce products to specifications acceptable to the FDA, EMA or other regulatory authorities, we may not obtain or maintain the approvals we need to commercialize such products. Even if we obtain regulatory approval for any of our product candidates, there is no assurance that either we or our third-party manufacturers will be able to manufacture the approved product to specifications acceptable to the FDA, EMA or other regulatory authorities, to produce it in sufficient quantities to meet the requirements for the potential launch of the product, or to meet potential future demand. Any of these challenges could delay initiation and completion of clinical trials, require bridging clinical trials or the repetition of one or more clinical trials, increase clinical trial costs, delay approval of our product candidate, impair commercialization efforts, increase our cost of goods, and have an adverse effect on our business, prospects, financial condition, results of operations and growth prospects.
| 68 |
Risks related to our Intellectual Property
We may not be able to protect our intellectual property rights throughout the world.
Filing, prosecuting and defending patents or establishing other intellectual property rights to our product candidates in all countries throughout the world would be prohibitively expensive, and our intellectual property rights in some countries outside the United States can be less extensive than those in the United States or non-existent. For example, the Melligen cells are protected by patents only in the U.S. and Europe and we are only pursuing patent protection for our pancreatic cancer product candidate in the U.S., Australia and Canada.
Many companies have encountered significant problems in protecting and defending intellectual property rights in foreign jurisdictions. The legal systems of some countries do not favor the enforcement of patents and other intellectual property protection, which could make it difficult for us to stop the infringement of our patents or misappropriation of our intellectual property rights generally. Proceedings to enforce our patent and other intellectual property rights in foreign jurisdictions could result in substantial costs and divert our efforts and attention from other aspects of our business, could put our patents or intellectual property rights at risk of being invalidated or interpreted narrowly and our patent applications at risk of not issuing and could provoke third parties to assert claims against us. We may not prevail in any lawsuits that we initiate, and the damages or other remedies awarded, if any, may not be commercially meaningful.
Many countries, including European Union countries, India, Japan and China, have compulsory licensing laws under which a patent owner may be compelled under specified circumstances to grant licenses to third parties. In those countries, we may have limited remedies if patents are infringed or if we are compelled to grant a license to a third party, which could materially diminish the value of those patents. This could limit our ability to pursue strategic alternatives, including identifying and consummating transactions with potential third-party partners, to further develop, obtain marketing approval for and/or commercialize our product candidates, and consequently our potential revenue opportunities.
Our intellectual property and data and market exclusivity may not be sufficient to block others from commercializing identical or competing products.
Our success depends in large part on our ability to obtain and maintain both intellectual property rights and data and market exclusivity for our product candidates in order to block others from commercializing identical or competing products. Establishing intellectual property rights includes filing, prosecuting, maintaining and enforcing patents that cover our product candidates and variations of our product candidates and protecting our trade secrets and other proprietary information related to our product candidates from unauthorized use.
The foundational patents relating to the Cell-in-the-Box® technology that were formerly licensed from Bavarian Nordic/GSF covering capsules encapsulating cells expressing cytochrome P450 and treatment methods using the same expired on March 27, 2017. Currently, we do not have any issued patents in any countries covering our product candidate for the treatment of pancreatic cancer. We exclusively license from UTS patented Melligen cells, which cover our product candidate for the treatment of diabetes, which are issued in the U.S. and Europe and expire in August 2028. Currently, we do not have any issued patents or pending applications covering our product candidate for the treatment of cancer using cannabinoids or our product candidate for the treatment of malignant ascites fluid therapy. We may not be able to obtain protection for our product candidates or variations of our product candidates. Even if our owned and licensed patent applications issue as patents, they may not issue in a form that will provide us with any meaningful protection, prevent competitors from competing with us or otherwise provide us with any competitive advantage or our patents may expire before or shortly after our product candidate is approved. Our competitors may be able to circumvent our owned or licensed patents by developing similar or alternative technologies or products in a non-infringing manner.
Confidential know-how and trade secrets are only protectable to the extent a third party utilizes the confidential know-how or trade secret in an unauthorized manner; however, if a third party is able to independently duplicate the technology, such as through reverse engineering, without access to or use of our confidential know-how or trade secret, we would have no recourse.
| 69 |
In addition, data exclusivity that is provided through the BPCIA in the U.S. and equivalents in foreign countries is limited in both time and scope. The BPCIA bars the FDA from approving biosimilar applications for 12 years after an innovator biological product receives initial marketing approval, however it does not bar the FDA from approving an identical or similar product that is the subject of its own BLA. Finally, upon the approval of the first BLA for a biologic designated as an Orphan Drug for a specified indication, the sponsor of that BLA is entitled to 7 years of exclusive marketing rights in the U.S. for biologic for the particular indication unless the sponsor cannot assure the availability of sufficient quantities to meet the needs of persons with the disease. In Europe, this exclusivity is 10 years. However, Orphan Drug status for an approved indication does not prevent another company from seeking approval of a biologic that has other labeled indications that are not under orphan or other exclusivities. In addition, in the U.S., the FDA is not prevented from approving another biologic for the same labeled Orphan indication if the company can demonstrate that the other biologic is clinically superior to first approved product.
Even if we are able to obtain patents, maintain confidential information, trade secrets, obtain data, and market exclusivity for our product candidates, our competitors may be able to develop and obtain approval of identical or competing products.
If we are unable to obtain and maintain intellectual property protection for our technology and product candidates, or if the scope of the intellectual property protection obtained is not sufficiently broad, our competitors could develop and commercialize technology and products similar or identical to ours, and our ability to successfully commercialize our technology and products may be impaired.
Our success depends in large part on our ability to obtain and maintain patent protection in the U.S. and other countries with respect to our proprietary technology and products. We seek to protect our proprietary position by filing patents in the U.S. and abroad related to our product candidates. Our patent portfolio relating to the Cell-in-the-Box® technology was formerly licensed from Bavarian Nordic/GSF. The Bavarian Nordic/GSF patents covered capsules encapsulating cells expressing cytochrome P450 and treatment methods using the same. These patents expired on March 27, 2017. We exclusively license from UTS patented Melligen cells, which cover our product candidate for the treatment of diabetes. The patents are issued in the U.S. and Europe and expire in August 2028. Currently, we do not have any issued patents in any countries covering our product candidate for the treatment of cancer; we have pending applications in the U.S., Australia and Canada and relating to our product candidate for the treatment of pancreatic cancer. If issued, such patents would expire in March 2038.
We cannot estimate the financial or other impact of the expiration of the Bavarian Nordic/GSF patents or the failure of the USPTO or similar regulatory authorities in other countries denying the claims we pursue in the U.S. and other countries.
The patent prosecution and/or patent maintenance process is expensive and time-consuming. We may not be able to file and prosecute or maintain all necessary or desirable patent applications or maintain the existing patents at a reasonable cost or in a timely manner. We may choose not to seek patent protection for certain innovations and may choose not to pursue patent protection in certain jurisdictions. Under the laws of certain jurisdictions, patents or other intellectual property rights may be unavailable or limited in scope. It is also possible that we will fail to identify patentable aspects of our discovery and preclinical development output before it is too late to obtain patent protection.
Moreover, in some circumstances, we do not have the right to control the preparation, filing and prosecution of patent applications, or to maintain the patents, covering technology that we license from third parties. Therefore, these patents and applications may not be prosecuted and enforced in a manner consistent with the best interests of our business.
The patent position of biotechnology and pharmaceutical companies generally is highly uncertain, involves complex legal and factual questions and has in recent years been the subject of much litigation. In addition, the laws of foreign countries may not protect our rights to the same extent as the laws of the U.S. For example, India does not allow patents for methods of treating the human body. Publications of discoveries in the scientific literature often lag the actual discoveries, and patent applications in the U.S. and other jurisdictions are typically not published until 18 or more months after filing, or in some cases not at all. Therefore, we cannot know with certainty whether we were the first to make the inventions claimed in our licensed patents or pending patent applications, or that we were the first to file for patent protection of such inventions. Consequently, the issuance, scope, validity, enforceability and commercial value of our patent rights are highly uncertain. Any future patent applications may not result in patents being issued which protect our technology or products, in whole or in part, or which effectively prevent others from commercializing competitive technologies and products. Changes in either the patent laws or interpretation of the patent laws in the U.S. and other countries may diminish the value of our patents or narrow the scope of our patent protection.
| 70 |
Patent reform legislation could increase the uncertainties and costs surrounding the prosecution of our owned or licensed patent applications and the enforcement or defense of our owned or licensed patents. On September 16, 2011, the Leahy-Smith America Invents Act (“Leahy-Smith Act”) was signed into law. The Leahy-Smith Act includes several significant changes to patent law in the U.S. These include provisions that affect the way patent applications are prosecuted and may also affect patent litigation. The USPTO recently developed new regulations and procedures to govern administration of the Leahy-Smith Act. Many of the substantive changes to patent law associated with the Leahy-Smith Act, such as the first to file provisions, only became effective on March 16, 2013. Accordingly, it is not clear what, if any, impact the Leahy-Smith Act will have on the operation of our business. However, the Leahy-Smith Act and its implementation could increase the uncertainties and costs surrounding the prosecution of our owned or licensed patent applications and the enforcement or defense of our owned or licensed patents, all of which could have a material adverse effect on our business and financial condition.
Also, we may be subject to a third-party pre-issuance submission of prior art to the USPTO, or become involved in opposition, derivation, reexamination, inter-party review, post-grant review or interference proceedings challenging our patent rights or the patent rights of others. An adverse determination in any such submission, proceeding or litigation could reduce the scope of, or invalidate, our patent rights, allow third parties to commercialize our technology or products and compete directly with us, without payment to us, or result in our inability to manufacture or commercialize products without infringing third-party patent rights. In addition, if the breadth or strength of protection provided by our patents and patent applications is threatened, it could dissuade companies from collaborating with us to license, develop or commercialize current our future product candidates.
Even if our owned and licensed patent applications issue as patents, they may not issue in a form that will provide us with any meaningful protection, prevent competitors from competing with us or otherwise provide us with any competitive advantage. Our competitors may be able to circumvent our owned or licensed patents by developing similar or alternative technologies or products in a non-infringing manner.
The issuance of a patent is not conclusive as to its inventorship, scope, validity or enforceability, and our owned and licensed patents may be challenged in the courts or patent offices in the U.S. and abroad. Such challenges may result in loss of exclusivity or freedom to operate or in patent claims being narrowed, invalidated or held unenforceable, in whole or in part, which could limit our ability to stop others from using or commercializing similar or identical technology and products, or limit the duration of the patent protection of our technology and products. Given the amount of time required for the development, testing and regulatory review of new product candidates, patents protecting such candidates might expire before or shortly after such candidates are commercialized. Thus, our owned and licensed patent portfolio may not provide us with sufficient rights to exclude others from commercializing products similar or identical to ours.
The risks described elsewhere pertaining to our patents and other intellectual property rights also apply to the intellectual property rights that we license, and any failure to obtain, maintain and enforce these rights could have a material adverse effect on our business. In some cases, we may not have control over the prosecution, maintenance or enforcement of the patents that we license. Moreover, our licensors may fail to take the steps that we believe are necessary or desirable to obtain, maintain and enforce the licensed patents. Any inability on our part to protect adequately our intellectual property may have a material adverse effect on our business, operating results and financial position.
If we do not obtain patent and/or data exclusivity for our product candidates, our business may be materially harmed.
Our commercial success will largely depend on our ability to obtain and maintain patent and other intellectual property protection and/or data exclusivity under the BPCIA in the U.S. and other countries with respect to our proprietary technology, product candidates and our target indications.
If we are unable to obtain patents covering our product candidates or obtain data and/or marketing exclusivity for our product candidates, our competitors may be able to take advantage of our investment in development and clinical trials by referencing our clinical and preclinical data to obtain approval of competing products, such as a biosimilar, earlier than might otherwise be the case.
| 71 |
Obtaining and maintaining our patent protection depends on compliance with various procedural, document submission, fee payment and other requirements imposed by governmental patent agencies. Our patent protection could be reduced or eliminated for non-compliance with these requirements.
Periodic maintenance fees, renewal fees, annuity fees and various other governmental fees on patents and/or applications will be due to be paid to the USPTO and various governmental patent agencies outside of the U.S. in several stages over the lifetime of the patents and/or applications. The USPTO and various non-U.S. governmental patent agencies require compliance with numerous procedural, documentary, fee payment and other similar provisions during the patent application process. We employ reputable law firms and other professionals to help us comply, and in many cases, an inadvertent lapse can be cured by payment of a late fee or by other means in accordance with the applicable rules. However, there are situations in which non-compliance can result in abandonment or lapse of the patent or patent application, resulting in partial or complete loss of patent rights in the relevant jurisdiction. In such an event, our competitors might be able to enter the market and this circumstance would have a material adverse effect on our business.
We may become involved in lawsuits to protect or enforce our patents or other intellectual property, which could be expensive, time consuming and unsuccessful.
Because competition in our industry is intense, competitors may infringe or otherwise violate our issued patents, patents of our licensors or other intellectual property. To counter infringement or unauthorized use, we may be required to file infringement claims, which can be expensive and time-consuming. Any claims we assert against perceived infringers could provoke these parties to assert counterclaims against us alleging that we infringe their patents. In addition, in a patent infringement proceeding, a court may decide that a patent of ours is invalid or unenforceable, in whole or in part, construe the patent’s claims narrowly or refuse to stop the other party from using the technology at issue because our patents do not cover the technology in question. An adverse result in any litigation proceeding could put one or more of the patents associated with our business at risk of being invalidated or interpreted narrowly. We may also elect to enter license agreements to settle patent infringement claims or to resolve disputes prior to litigation, and any such license agreements may require us to pay royalties and other fees that could be significant. Furthermore, because of the substantial amount of discovery required in intellectual property litigation, there is a risk that some of our confidential information could be compromised by disclosure.
If we breach any of our license or collaboration agreements, it could compromise our development and commercialization efforts for our product candidates.
We have licensed rights to intellectual property from third parties to commercialize our product candidates, including our Cell-in-a-Box® Technology for LAPC and diabetes and our COVID-19 diagnostic kits. If we materially breach or fail to perform any provision under these license and collaboration agreements, including failure to make payments to a licensor or collaborator when due for royalties and failure to use commercially reasonable efforts to develop and commercialize our product candidates, such licensors and collaborators have the right to terminate our agreements, and upon the effective date of such termination, our right to practice the licensed intellectual property would end. Any uncured, material breach under the agreements could result in our loss of rights to practice the patent rights and other intellectual property licensed to us under the agreements and could result in the loss of our ability to develop or commercialize our product candidates.
We may need to license certain intellectual property from third parties, and such licenses may not be available or may not be available on commercially reasonable terms.
A third party may hold intellectual property, including patent rights, which are important or necessary to the development of our products. It may be necessary for us to use the patented or proprietary technology of third parties to commercialize our products, in which case we would be required to obtain a license from these third parties on commercially reasonable terms, or our business could be harmed, possibly materially. Although we believe that licenses to these patents may be available from these third parties on commercially reasonable terms, if we were not able to obtain a license, or are not able to obtain a license on commercially reasonable terms, our business could be harmed, possibly materially.
| 72 |
Third parties may initiate legal proceedings alleging that we are infringing their intellectual property rights, the outcome of which would be uncertain and could have a material adverse effect on the success of our business.
Our commercial success depends upon our ability, and the ability of our collaborators, to develop, manufacture, market and sell our product candidates and use our proprietary technologies without infringing the proprietary rights of third parties. There is considerable intellectual property litigation in the biotechnology and pharmaceutical industries. We may become party to, or threatened with, future adversarial proceedings or litigation regarding intellectual property rights with respect to our products and technology, including interference or derivation proceedings before the USPTO and various governmental patent agencies outside of the U.S. Third parties may assert infringement claims against us based on existing patents or patents that may be granted in the future.
If we are found to infringe a third party’s intellectual property rights, we could be required to obtain a license from such third party to continue developing and marketing our product candidates and technology. However, we may not be able to obtain any required license on commercially reasonable terms or at all. Even if we could obtain a license, it could be non-exclusive, thereby giving our competitors access to the same technologies licensed to us. We could be forced, including by court order, to cease commercializing the infringing technology or product. In addition, we could be found liable for monetary damages, including treble damages and attorneys’ fees if we are found to have willfully infringed a patent. A finding of infringement could prevent us from commercializing our product candidates or force us to cease some of our business operations, which could materially harm our business. Claims that we have misappropriated the confidential information or trade secrets of third parties could have a similar negative impact on our business.
We may not be successful in obtaining or maintaining necessary rights for its development pipeline through acquisitions and licenses from third parties.
Because our programs may involve additional product candidates that may require the use of proprietary rights held by third parties, the growth of our business may depend in part on our ability to acquire, in-license or use these proprietary rights. We may be unable to acquire or in-license any compositions, methods of use or other third-party intellectual property rights from third parties that we identify. The licensing and acquisition of third-party intellectual property rights is a competitive area, and numerous established companies are also pursuing strategies to license or acquire third-party intellectual property rights that we may consider attractive. These established companies may have a competitive advantage over us due to their size, cash resources and greater clinical development and commercialization capabilities.
In addition, companies that perceive us to be a competitor may be unwilling to assign or license rights to us. We also may be unable to license or acquire third-party intellectual property rights on terms that would allow us to make an appropriate return on our investment. If we are unable to successfully obtain rights to required third-party intellectual property rights, our business, financial condition and prospects for growth could suffer.
If we are unable to protect the confidentiality of our trade secrets, our business and competitive position would be harmed.
In addition to seeking patents for some of our technology and product candidates, we also rely on trade secrets, including unpatented know-how, technology and other proprietary information, to maintain our competitive position. We seek to protect these trade secrets, in part, by entering non-disclosure and confidentiality agreements with parties who have access to them, such as our employees, corporate collaborators, outside scientific collaborators, contract manufacturers, consultants, advisors and other third parties. We seek to protect our confidential proprietary information, in part, by entering confidentiality agreements with our employees and consultants; however, we cannot be certain that such agreements have been entered with all relevant parties.
Moreover, to the extent we enter such agreements, any of these parties may breach the agreements and disclose our proprietary information, including our trade secrets to unaffiliated third parties. We may not be able to obtain adequate remedies for such breaches. Enforcing a claim that a party illegally disclosed or misappropriated a trade secret is difficult, expensive and time-consuming and the outcome is unpredictable. In addition, some courts inside and outside the U.S. are less willing or unwilling to protect trade secrets. If any of our trade secrets were to be lawfully obtained or independently developed by a competitor, we would have no right to prevent them, or those to whom they communicate them, from using that technology or information to compete with us. If any of our trade secrets were to be disclosed to or independently developed by a competitor, our competitive position would be harmed.
| 73 |
The majority of the technology that we license and use for our product candidates is not protected by patents, but rather is based upon confidential know-how and trade secrets. Confidential know-how and trade secrets are only protectable to the extent a third party utilizes the confidential know-how or trade secret in an unauthorized manner; however, if a third party is able to independently duplicate the technology, such as through reverse engineering, without access to or use of our confidential know-how or trade secret, we would have no recourse.
We may be subject to claims that our employees, consultants or independent contractors have wrongfully used or disclosed confidential information of their former employers or other third parties.
We employ individuals and use consultants and independent contractors who were previously employed at other biotechnology or pharmaceutical companies. Although we seek to ensure that our employees and our consultants and independent contractors do not use the proprietary information or know-how of others in their work for us, we may be subject to claims that we or our employees, consultants or independent contractors have inadvertently or otherwise used or disclosed trade secrets, or other confidential information of our employees’, consultants’ or independent contractors’ former employers, clients or other third parties. We may also be subject to claims that former employers or other third parties have an ownership interest in our patents. Litigation may be necessary to defend against these claims. There is no guarantee of success in defending these claims, and if we fail in defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights, such as exclusive ownership of, or right to use, valuable intellectual property. Even if we are successful, litigation could result in substantial cost and be a distraction to our management and others working for us.
In addition, while it is our policy to require our employees, consultants and independent contractors who may be involved in the development of intellectual property to execute agreements assigning such intellectual property to us, we may be unsuccessful in executing such an agreement with each party who in fact develops intellectual property that we regard as our own. Our and their assignment agreements may not be self-executing or may be breached, and we may be forced to bring claims against third parties, or defend claims they may bring against us, to determine the ownership of what we regard as our intellectual property. If we or our licensors fail in prosecuting or defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights or personnel. Even if we and our licensors are successful in prosecuting or defending against such claims, litigation could result in substantial costs and be a distraction to management.
Any trademarks we have obtained or may obtain may be infringed or successfully challenged, resulting in harm to our business.
We expect to rely on trademarks as one means to distinguish any of our drug candidates that are approved for marketing from the products of our competitors. Once we select new trademarks and apply to register them, our trademark applications may not be approved. Third parties may oppose or attempt to cancel our trademark applications or trademarks, or otherwise challenge our use of the trademarks. If our trademarks are successfully challenged, we could be forced to rebrand our drugs, which could result in loss of brand recognition and could require us to devote resources to advertising and marketing new brands. Our competitors may infringe our trademarks and we may not have adequate resources to enforce our trademarks.
Intellectual property rights do not necessarily address all potential threats to our competitive advantage.
The degree of future protection afforded by our intellectual property rights is uncertain because intellectual property rights have limitations, and may not adequately protect our business, or permit us to maintain our competitive advantage. The following examples are illustrative:
| · | others may be able to make compositions that are the same as or like our product candidates, but that are not covered by the claims of any patents that we may own or exclusively license; | |
| · | others may be able to make product that is like the product candidates we intend to commercialize that is not covered by any patents that we might own or exclusively license and have the right to enforce; | |
| · | we, our licensors or any collaborators might not have been the first to make the inventions covered by issued patents or pending patent applications that we may own; | |
| · | we, our licensors or any collaborators might not have been the first to file patent applications covering certain of our inventions; | |
| · | others may independently develop similar or alternative technologies or duplicate any of our technologies without infringing our intellectual property rights; | |
| · | it is possible that our pending patent applications will not lead to issued patents; | |
| · | issued patents that we may own may not provide us with any competitive advantages, or may be held invalid or unenforceable because of legal challenges; | |
| · | our competitors might conduct research and development activities in the U.S. and other countries that provide a safe harbor from patent infringement claims for certain research and development activities, as well as in countries where we do not have patent rights, and then use the information learned from such activities to develop competitive products for sale in our major commercial markets; and | |
| · | we may not develop additional proprietary technologies that are patentable. |
| 74 |
Additional Risks Related to Our Business Model and Operations
Development of brand awareness is critical to our success.
For certain market segments that we plan to pursue, the development of our brand awareness is essential for us to reduce our marketing expenditures over time and realize greater benefits from marketing expenditures. If our brand-marketing efforts are unsuccessful, growth prospects, financial condition and results of operations would be adversely affected. Our brand awareness efforts have required, and will most likely continue to require, additional expenses and time of the current senior management team.
Any weakness in our internal controls could have a material adverse effect on us.
As discussed in Item 9A. “Controls and Procedures,” the senior management has identified a material weakness in our internal controls over financial reporting and cannot assure you that additional material weaknesses will not be identified in the future. We cannot assure you that these steps will be successful in preventing material weaknesses or significant deficiencies in our internal controls over financial reporting in the future. In addition, any such failure could adversely affect our ability to report financial results on a timely and accurate basis, which could have other material effects on our business, reputation, results of operations, financial condition or liquidity. Material weaknesses in internal controls over financial reporting or disclosure controls and procedures could also cause investors to lose confidence in our reported financial information which could have an adverse effect on the trading price of our securities.
The success of our cannabis program may depend on additional states legalizing medical Cannabis.
Continued development of the medical Cannabis market is dependent upon continued legislative authorization of Cannabis at the state level for medical purposes. Any number of factors could slow or halt the progress. Further, progress, while encouraging, is not assured and the process normally encounters setbacks before achieving success. While there may be ample public support for legislative proposal, key support must be created in the legislative committee, or a bill may never advance to a vote. Numerous factors impact the legislative process. Any one of these factors could slow or halt the progress and adoption of Cannabis for medical purposes, which would limit the market for our product candidates that are based on Cannabis constituents and negatively impact our business in this area.
Medicinal Cannabis faces strong opposition.
Certain well-funded and significant businesses may have a strong economic opposition to the medical Cannabis industry. Lobbying by groups within the pharmaceutical industry or changes in the regulation of Cannabis-based therapies could affect our ability to develop and market cannabinoid-based cancer therapies.
Our product candidates involving Cannabis will be subject to controlled substance laws and regulations. Failure to receive necessary approvals may delay the launch of our products and failure to comply with these laws and regulations may adversely affect the results of our business operations.
Our product candidates involving Cannabis contain controlled substances as defined in the CSA. Controlled substances that are pharmaceutical products are subject to a high degree of regulation under the CSA, which establishes, among other things, certain registration, manufacturing quotas, security, recordkeeping, reporting, import, export and other requirements administered by the DEA. The DEA classifies controlled substances into five schedules: Schedule I, II, III, IV or V substances. Schedule I substances by definition have a high potential for abuse, have not currently “accepted medical use” in the U.S., lack accepted safety for use under medical supervision, and may not be prescribed, marketed or sold in the U.S. Pharmaceutical products approved for use in the U.S. may be listed as Schedule II, III, IV or V, with Schedule II substances considered to present the highest potential for abuse or dependence and Schedule V substances the lowest relative risk of abuse among such substances. Schedule I and II drugs are subject to the strictest controls under the CSA, including manufacturing and procurement quotas, security requirements and criteria for importation. In addition, dispensing of Schedule II drugs is further restricted. For example, they may not be refilled without a new prescription.
| 75 |
While Cannabis is a Schedule I controlled substance, products approved for medical use in the U.S. that contain Cannabis or Cannabis extracts must be placed in Schedules II - V, since approval by the FDA satisfies the “accepted medical use” requirement. If we receive FDA approval for a product candidate involving Cannabis, the DEA will make a scheduling determination and place it in a schedule other than Schedule I for it to be prescribed to patients in the U.S. If approved by the FDA, we expect the product candidates to be listed by the DEA as a Schedule II or III controlled substance. Consequently, their manufacture, importation, exportation, domestic distribution, storage, sale and legitimate use will be subject to a significant degree of regulation by the DEA. The scheduling process may take one or more years beyond FDA approval, thereby significantly delaying the launch of our product candidates involving Cannabis. Furthermore, if the FDA, DEA or any foreign regulatory authority determines that our product candidates involving Cannabis may have potential for abuse, it may require us to generate more clinical data than that which is currently anticipated, which could increase the cost and/or delay the launch of such products.
Because one or more of our product candidates contain active ingredients of Cannabis, which are Schedule I substances, to conduct preclinical studies and clinical trials with these product candidates in the U.S. prior to approval, each of our research sites must submit a research protocol to the DEA and obtain and maintain a DEA researcher registration that will allow those sites to handle and dispense our product candidates and to obtain the product from our manufacturer. If the DEA delays or denies the grant of a research registration to one or more research sites, the preclinical studies or clinical trials could be significantly delayed, and we could lose and be required to replace clinical trial sites, resulting in additional costs.
Individual states have also established controlled substance laws and regulations. Though state-controlled substance laws often mirror federal law because the states are separate jurisdictions, they may separately schedule our product candidates involving Cannabis as well. While some states automatically schedule a drug based on federal action, other states schedule drugs through rulemaking or a legislative action. State scheduling may delay commercial sale of any product for which we obtain federal regulatory approval and adverse scheduling could have a material adverse effect on the commercial attractiveness of such product. We or our partners must also obtain separate state registrations, permits or licenses to be able to obtain, handle, and distribute controlled substances for clinical trials or commercial sale, and failure to meet applicable regulatory requirements could lead to enforcement and sanctions by the states in addition to those from the DEA or otherwise arising under federal law.
Because of these risks, no assurance can be given that our Cannabis therapy under development will be successful.
The insurance coverage and reimbursement status of newly approved products are uncertain. Failure to obtain or maintain adequate coverage and reimbursement for new or current products could limit our ability to market those products and decrease our ability to generate revenue.
The availability and extent of reimbursement by governmental and private payors is essential for most patients to be able to afford expensive treatments. Sales of our products, if approved will depend substantially, both domestically and abroad, on the extent to which the costs of our products, if approved, will be paid by health maintenance, managed care, pharmacy benefit and similar healthcare management organizations, or reimbursed by government health administration authorities, private health coverage insurers and other third-party payors. If reimbursement is not available, or is available only to limited levels, we may not be able to successfully commercialize our product candidates. Even if coverage is provided, the approved reimbursement amount may not be high enough to allow us to establish or maintain pricing sufficient to realize a sufficient return on our investment.
There is significant uncertainty related to the insurance coverage and reimbursement of newly approved products. In the U.S., the principal decisions about reimbursement for new medicines are typically made by the CMS, an agency within the HHS. CMS decides whether and to what extent a new medicine will be covered and reimbursed under Medicare. Private payors tend to follow CMS to a substantial degree. It is difficult to predict what CMS will decide with respect to reimbursement for fundamentally novel products such as ours, as there is no body of established practices and precedents for these new products. Reimbursement agencies in Europe may be more conservative than CMS. For example, several cancer drugs have been approved for reimbursement in the U.S. and have not been approved for reimbursement in certain European countries. Outside the U.S., international operations are generally subject to extensive governmental price controls and other market regulations, and we believe the increasing emphasis on cost-containment initiatives in Europe, Canada and other countries has and will continue to put pressure on the pricing and usage of our product candidates. In many countries, the prices of medical products are subject to varying price control mechanisms as part of national health systems. In general, the prices of medicines under such systems are substantially lower than in the U.S. Other countries allow companies to fix their own prices for medicines but monitor and control company profits. Additional foreign price controls or other changes in pricing regulation could restrict the amount that we can charge for our product candidates. Accordingly, in markets outside the U.S., the reimbursement for our products may be reduced compared with the U.S. and may be insufficient to generate commercially reasonable revenues and profits.
| 76 |
Moreover, increasing efforts by governmental and third-party payors, in the U.S. and abroad, to cap or reduce healthcare costs may cause such organizations to limit both coverage and level of reimbursement for new products approved and, thus, they may not cover or provide adequate payment for our product candidates. We expect to experience pricing pressures with the sale of any of our products, if approved, due to the trend toward managed healthcare, the increasing influence of health maintenance organizations and additional legislative changes. The downward pressure on healthcare costs in general, particularly prescription drugs and biologics and surgical procedures and other treatments, has become very intense. Because of this, increasingly high barriers are being erected to the entry of new products into the healthcare market.
In addition to CMS and private payors, professional organizations such as the National Comprehensive Cancer Network and the American Society of Clinical Oncology can influence decisions about reimbursement for new medicines by determining standards for care. Many private payors may also contract with commercial vendors who sell software that provide guidelines that attempt to limit utilization of, and therefore reimbursement for, certain products deemed to provide limited benefit to existing alternatives. Such organizations may set guidelines that limit reimbursement or utilization of our products.
Our employees, consultants and independent contractors may engage in misconduct or other improper activities, including noncompliance with regulatory standards and requirements, which could subject us to significant liability and harm our reputation.
We are exposed to the risk of fraud and other misconduct by those who work for us. Misconduct by employees, consultants or independent contractors could include failures to comply with the FCPA or with the DEA, the FDA or the EMA regulations or similar regulations of other foreign regulatory authorities or to provide accurate information to the DEA, the FDA, the EMA or other foreign regulatory authorities. In addition, misconduct could include failures to comply with certain manufacturing standards, to comply with U.S. federal and state healthcare fraud and abuse laws and regulations and similar laws and regulations established and enforced by comparable foreign regulatory authorities, to report financial information or data accurately or to disclose unauthorized activities to us. Misconduct by those who work for us could also involve the improper use of information obtained during our clinical trials, which could result in regulatory sanctions and serious harm to our reputation. We have implemented and will enforce a Code of Business Conduct and Ethics, but it is not always possible to identify and deter misconduct by those who work for us. The precautions we take to detect and prevent this activity may not be effective in controlling unknown or unmanaged risks or losses or in protecting us from governmental investigations or other actions or lawsuits stemming from a failure to comply with such laws or regulations. If any such actions are instituted against us, and we are not successful in defending ourselves or asserting our rights, those actions could have a significant impact on our business and results of operations, including the imposition of significant fines or other sanctions.
Our transactions and relationships outside the U.S. will be subject to the FCPA and similar anti-bribery and anti-corruption laws.
As we pursue international clinical trials, licensing and, in the future, sales arrangements outside the U.S., we will be heavily regulated and expect to have significant interaction with foreign officials. Additionally, in many countries outside the U.S., the health care providers who prescribe pharmaceuticals are employed by the government and the purchasers of pharmaceuticals are government entities; therefore, our interactions with these prescribers and purchasers would be subject to regulation under the FCPA and similar anti-bribery or anti-corruption laws, regulations or rules of other countries in which we operate. The FCPA generally prohibits paying, offering or authorizing payment or offering of anything of value, directly or indirectly, to any foreign official, political party or candidate to influence official action, or otherwise obtain or retain business. The FCPA also requires public companies to make and keep books and records that accurately and fairly reflect the transactions of the corporation and to devise and maintain an adequate system of internal accounting controls.
Compliance with these laws and regulations may be costly and may limit our ability to expand into certain markets. There is no certainty that all our employees, agents, contractors, or collaborators, or those of our affiliates, will comply with all applicable laws and regulations, particularly given the high level of complexity of these laws and regulations. Violations of these laws and regulations could result in fines, criminal sanctions against us, our officers, or our employees, the closing down of our facilities, requirements to obtain export licenses, cessation of business activities in sanctioned countries, implementation of compliance programs and prohibitions on the conduct of our business. Any such violations could include prohibitions on our ability to offer our products in one or more countries and could materially damage our reputation, our brand, our international expansion efforts, our ability to attract and retain employees and our business, prospects, operating results and financial condition.
| 77 |
Product liability lawsuits against us could cause us to incur substantial liabilities and to limit commercialization of any products that we may develop.
We face an inherent risk of product liability exposure related to the testing of our product candidates in human clinical trials and will face an even greater risk if we commercially sell any products that we may develop. If we cannot successfully defend ourselves against claims that our product candidates or products caused injuries, we will incur substantial liabilities. Regardless of merit or eventual outcome, liability claims may result in:
| · | Decreased demand for any product candidates or products that we may develop; | |
| · | Injury to our reputation and significant negative media attention; | |
| · | Withdrawal of clinical trial participants; | |
| · | Significant costs to defend the related litigation; | |
| · | Substantial monetary awards to trial participants or patients; | |
| · | Loss of revenue; | |
| · | Reduced resources of our management to pursue our business strategy; and | |
| · | The inability to commercialize any products that we may develop. |
We currently do not have product liability insurance because we do not have any products to market. We will need such insurance for clinical trials, if allowed to proceed, and for commercialization of our products, if approved. Product liability insurance coverage is increasingly expensive. We may not be able to maintain insurance coverage at a reasonable cost or in an amount adequate to satisfy any liability that may arise.
We incur increased costs because of operating as a public company, and our management is required to devote substantial time to new compliance initiatives.
As a public company, we have incurred and are continuing to incur significant legal, accounting and other expenses. These expenses may increase. We are subject to, among others, the reporting requirements of the Exchange Act of 1934, as amended (“Exchange Act”), the Sarbanes-Oxley Act, the Dodd-Frank Wall Street Reform and Protection Act, as well as rules adopted, and to be adopted, by the Commission. Our management and other personnel devote a substantial amount of time to these compliance initiatives.
Moreover, these rules and regulations have substantially increased our legal and financial compliance costs and made some activities more time-consuming and costlier. The increased costs have increased our net loss. These rules and regulations may make it more difficult and more expensive for us to maintain sufficient director and officer liability insurance coverage. We cannot predict or estimate the amount or timing of additional costs we may continue to incur to respond to these requirements. The ongoing impact of these requirements could also make it more difficult for us to attract and retain qualified persons to serve on our Board, our Board committees or as executive officers.
Risk Factors Related to Our Stock and Financial Condition
Our common stock is currently listed on Nasdaq. Market prices for our shares of common stock will be influenced by several factors, including, but not limited to:
| · | The issuance of new shares pursuant to future offering; | |
| · | Changes in interest rates; | |
| · | New services or significant contracts and acquisitions; | |
| · | Variations in quarterly operating results; | |
| · | Change in financial estimates by securities analysts; | |
| · | The depth and liquidity of the market for the shares; | |
| · | Investor perceptions of us and of investments based in the countries where we do business or conduct research; and | |
| · | General economic and other national and international conditions. |
| 78 |
You may experience future dilution as a result of future equity offerings.
In order to raise additional capital, we may in the future offer additional common stock or other securities convertible into or exchangeable for our common stock at prices lower than that paid by existing investors. Investors purchasing shares or other securities in the future could have rights superior to existing shareholders. The price per share at which we sell additional shares of our common stock, or securities convertible or exchangeable into common stock, in future transactions may be higher or lower than the price per share paid by existing investors.
We may not be able to meet the continued listing requirements for Nasdaq or another nationally recognized stock exchange, which could limit investors’ ability to make transactions in our securities and subject us to additional trading restrictions.
In order to remain listed on Nasdaq, we will be required to meet the continued listing requirements of Nasdaq or any other U.S. or nationally recognized stock exchange to which we may apply and be approved for listing. We may be unable to satisfy these continued listing requirements, and there is no guarantee that our common stock will remain listed on Nasdaq or any other U.S. or nationally recognized stock exchange. If, after listing, our common stock is delisted from Nasdaq or any other U.S. or nationally recognized stock exchange, we could face significant material adverse consequences, including:
| · | a limited availability of market quotations for our common stock; |
| · | reduced liquidity with respect to the market for our common stock; |
| · | a determination that our common stock is a “penny stock,” which will require brokers trading in our common stock to adhere to different rules, possibly resulting in a reduced level of trading activity in the secondary trading market for our common stock; |
| · | a limited amount of news and analyst coverage; and |
| · | decreased ability to issue additional shares of our common stock or obtain additional financing in the future. |
We cannot assure you that we will be able to continue to comply with the minimum bid price requirement of Nasdaq.
There can be no assurance that the market price of our common stock will remain at the level required for continuing compliance with Nasdaq’s minimum bid requirement. It is not uncommon for the market price of a company’s common stock to decline in the period following a reverse stock split. If the market price of our common stock declines following the effectuation of the reverse stock split, the percentage decline may be greater than would occur in the absence of a reverse stock split. In any event, other factors unrelated to the number of shares of our common stock outstanding, such as negative financial or operational results, could adversely affect the market price of our common stock and jeopardize our ability to maintain compliance with Nasdaq’s minimum bid price requirement.
There can be no assurance that we will be able to comply with the continued listing standards of Nasdaq, a failure of which could result in a de-listing of our common stock.
Nasdaq requires that the trading price of its listed stocks remain above one dollar in order for the stock to remain listed. It is not uncommon for the market price of a company’s common stock to decline in the period following a reverse stock split. If the market price of our common stock declines following the effectuation of the reverse stock split, the percentage decline may be greater than would occur in the absence of a reverse stock split. In any event, other factors unrelated to the number of shares of our common stock outstanding, such as negative financial or operational results, could adversely affect the market price of our common stock and jeopardize our ability to maintain compliance with Nasdaq’s minimum bid price requirement. If a listed stock trades below one dollar for more than 30 consecutive trading days, then it is subject to delisting from Nasdaq. In addition, to maintain a listing on Nasdaq, we must satisfy minimum financial and other continued listing requirements and standards, including those regarding director independence and independent committee requirements, minimum stockholders’ equity and certain corporate governance requirements. If we are unable to satisfy these requirements or standards, we could be subject to delisting. This would have a negative effect on the price of our common stock and would impair your ability to sell or purchase our common stock when you wish to do so. In the event of a delisting, we can provide no assurance that any action we may take to restore our compliance with the listing requirements would allow our common stock to become listed again, stabilize the market price or improve the liquidity of our common stock, prevent our common stock from dropping below the minimum bid price requirement, or prevent future non-compliance with the listing requirements.
| 79 |
Since our common stock is listed on Nasdaq, we will incur materially increased costs and become subject to additional regulations and requirements.
Since our common stock was recently listed on Nasdaq, we will incur material legal, accounting and other expenses, including payment of annual exchange fees, to satisfy the continued listing standards for Nasdaq. If our common stock is listed on Nasdaq, we must meet certain financial and liquidity criteria to maintain our listing. If we fail to meet any of Nasdaq’s listing standards, our common stock may be delisted. In addition, our Board may determine that the cost of maintaining our listing on a national securities exchange outweighs the benefits of such listing. A delisting of our common stock from Nasdaq may materially impair our stockholders’ ability to buy and sell our common stock and could have an adverse effect on the market price of, and the efficiency of the trading market for, our common stock. The delisting of our common stock could significantly impair our ability to raise capital and the value of your investment.
A large number of shares may be issued and subsequently sold upon the exercise of existing options and warrants.
As of July 25, 2022, there were 769,129 shares of common stock issuable under outstanding options and 9,890,847 shares issuable upon exercise of outstanding warrants at various exercise prices. To the extent that holders of existing options or warrants sell the shares of common stock issued upon the exercise of warrants, the market price of our common stock may decrease due to the additional selling pressure in the market. The risk of dilution from issuances of shares of common stock underlying existing options and warrants may cause shareholders to sell their common stock, which could further decline in the market price. In addition, we will be issuing Common Warrants to purchase shares of common stock which are immediately exercisable.
We may experience volatility in our stock price, which may adversely affect the trading price of our common stock.
We have experienced significant volatility from time to time in the market price of our shares of common stock. Factors that may affect the market price include the following:
| · | Announcements of regulatory developments or technological innovations by us or our competitors; | |
| · | Changes in our relationship with our licensors and other strategic partners; | |
| · | Our quarterly operating results; | |
| · | Litigation involving or affecting us; | |
| · | Shortfalls in our actual financial results compared to our guidance or the forecasts of stock market analysts; | |
| · | Developments in patent or other technology ownership rights; | |
| · | Acquisitions or strategic alliances by us or our competitors; | |
| · | Public concern regarding the safety of our products; and | |
| · | Government regulation of drug pricing. |
The price of our common stock is volatile, which substantially increases the risk that our investors may not be able to sell their shares at or above the price that the investors have paid for their shares.
Because of the price volatility in our shares, we have observed since its inception, investors in our common stock may not be able to sell their shares when they desire to do so at a price the investors desire to attain. Over the past twelve months, shares of our common stock were quoted and traded at a high of $27.16 per share and a low of $1.79 per share. The inability to sell securities in a rapidly declining market may substantially increase the risk of loss because the price of our common stock may suffer greater declines due to the historical price volatility of our shares. Certain factors, some of which are beyond our control, which may cause our share price to fluctuate significantly include, but are not limited to, the following:
| · | Variations in our quarterly operating results; | |
| · | Loss of a key relationship or failure to complete significant product candidate milestones timely or at all; | |
| · | Additions or departures of key personnel; and | |
| · | Fluctuations in the stock market price and volume. |
| 80 |
In addition, in recent years the stock market in general, and the over-the-counter markets in particular, have experienced extreme price and volume fluctuations. In some cases, these fluctuations are unrelated or disproportionate to the performance of the underlying company. These market and industry factors may materially and adversely affect our share price, regardless of our performance or whether we meet our business objectives. In the past, class action litigation often has been brought against companies following periods of volatility in the market price of those companies’ common stock. If we become involved in this type of litigation in the future, it could result in substantial costs and diversion of management attention and resources, which could have a material adverse effect on us and the trading price of our common stock.
We have no plans to pay dividends in the foreseeable future, and investors may not expect a dividend as a return of or on any investment in us.
We have not paid dividends on our shares of common stock and do not anticipate paying such dividends in the foreseeable future.
We are a “smaller reporting company” under the SEC’s disclosure rules and have elected to comply with the reduced disclosure requirements applicable to smaller reporting companies.
We are a “smaller reporting company” under the SEC’s disclosure rules, meaning that we have either:
| · | a public float of less than $250 million; or |
| · | annual revenues of less than $100 million during the most recently completed fiscal year; and |
| · | no public float; or |
| · | a public float of less than $700 million. |
As a smaller reporting company, we are permitted to comply with scaled-back disclosure obligations in our SEC filings compared to other issuers, including with respect to disclosure obligations regarding executive compensation in our periodic reports and proxy statements. We have elected to adopt the accommodations available to smaller reporting companies. Until we cease to be a smaller reporting company, the scaled-back disclosure in our SEC filings will result in less information about our company being available than for other public companies.
If investors consider our common stock less attractive as a result of our election to use the scaled-back disclosure permitted for smaller reporting companies, there may be a less active trading market for our common stock and our share price may be more volatile.
As a non-accelerated filer, we are not required to comply with the auditor attestation requirements of the Sarbanes-Oxley Act.
We are a non-accelerated filer under the Securities Exchange Act of 1934, as amended, or the Exchange Act, and we are not required to comply with the auditor attestation requirements of Section 404(b) of the Sarbanes-Oxley Act of 2002. Therefore, our internal controls over financial reporting will not receive the level of review provided by the process relating to the auditor attestation included in annual reports of issuers that are subject to the auditor attestation requirements. In addition, we cannot predict if investors will find our common stock less attractive because we are not required to comply with the auditor attestation requirements. If some investors find our common stock less attractive as a result, there may be a less active trading market for our common stock and trading price for our common stock may be negatively affected.
| 81 |
Risks Related to Employee and Tax Matters, Managing Growth and Macroeconomic Conditions
We have a limited number of employees and are highly dependent on our Chief Executive Officer and Chief Financial Officer. Our future success depends on our ability to retain these officers and other key personnel and to attract, retain and motivate other needed qualified personnel.
We are an early-stage biotechnology company with a limited operating history. As of April 30, 2022, we had 4 full-time employees and 23 consultants. We are highly dependent on the R&D, clinical and business development expertise of the principal members of our management, scientific and clinical teams, specifically, on our Chief Executive Officer and Chief Financial Officer. Recruiting and retaining qualified scientific, clinical, manufacturing and sales and marketing personnel will also be critical to our success. The loss of the services of our Chief Executive Officer and Chief Financial Officer or other key employees or consultants could severely impede the achievement of our R&D and commercialization of our product candidates and seriously harm our ability to successfully implement our business strategy.
Furthermore, replacing executive officers and key employees and consultants may be difficult and may take an extended period because of the limited number of individuals in our industry with the breadth of skills and experience required to successfully develop, gain regulatory approval of and commercialize our product candidates. Competition to hire from this limited pool is intense, and we may be unable to hire, train, retain or motivate these key personnel on acceptable terms given the competition among numerous pharmaceutical and biotechnology companies for similar personnel.
We also experience competition for the hiring of scientific and clinical personnel from universities and research institutions. In addition, we rely on other consultants and advisors, including scientific and clinical advisors, to assist us in formulating our discovery, preclinical and clinical development and commercialization strategy. Our consultants and advisors may be employed by employers other than us and may have commitments under consulting or advisory contracts with other entities that may limit their availability to us. If we are unable to continue to attract and retain high quality personnel, our ability to pursue our growth strategy will be limited.
Our ability to use our net operating loss carryforwards and certain other tax attributes may be limited.
As of April 30, 2022, we had federal net operating loss carryforwards of approximately $62 million, which will begin to expire in varying amounts beginning in 2022. Under Sections 382 and 383 of the United States Internal Revenue Code of 1986, as amended, or the Code, and corresponding provisions of state law, if a corporation undergoes an “ownership change,” (generally defined as a greater than 50-percentage-point cumulative change (by value) in the equity ownership of certain stockholders over a rolling three-year period), the corporation’s ability to use its pre-change net operating loss carryforwards and other pre-change tax attributes to offset its post-change taxable income or taxes may be limited.
We may have experienced ownership changes in the past and could experience one or more ownership changes in the future, some of which are outside our control. Our net operating loss carryforwards may also be subject to limitation under state laws. Further, our ability to utilize net operating loss carryforwards of companies that we may acquire in the future may also be subject to limitations. There is also a risk that due to tax law changes, such as suspensions on the use of net operating loss carryforwards, or other unforeseen reasons, our ability to use our pre-change net operating loss carryforwards and other pre-change tax attributes to offset post-change taxable income or taxes may be subject to limitation or expire.
We expect to expand our development and regulatory capabilities and potentially implement sales, marketing and distribution capabilities. Thus, we may encounter difficulties in managing our growth, which could disrupt our operations.
We expect to experience significant growth in the number of our employees and the scope of our operations, particularly in the areas of drug development, regulatory affairs and, if any of our product candidates receive marketing approval, sales, marketing and distribution. To manage our anticipated future growth, we must continue to implement and improve our managerial, operational and financial systems, expand our facilities and continue to recruit and train additional qualified personnel. Due to our limited financial resources and the limited experience of our management team in managing a company with such anticipated growth, we may not be able to effectively manage the expansion of our operations or recruit and train additional qualified personnel. The expansion of our operations may lead to significant costs and may divert our management and business development resources. Any inability to manage growth could delay the execution of our business plans or disrupt our operations.
| 82 |
Unfavorable global economic conditions could adversely affect our business, financial condition or results of operations.
Our results of operations could be adversely affected by general conditions in the global economy and in the global financial markets. The recent global financial crisis related to COVID-19 caused extreme volatility and disruptions in the capital and credit markets. A severe or prolonged economic downturn, such as the recent global financial crisis, could result in a variety of risks to our business, including our ability to raise additional capital when needed on acceptable terms, if at all. A weak or declining economy could also strain our suppliers, possibly resulting in supply disruption. Any of the foregoing could adversely impact our business.
Our business and operations would suffer in the event of system failures.
Despite the implementation of security measures, our internal computer systems and those of our third-party service providers on whom we rely on are vulnerable to damage from computer viruses, unauthorized access, natural disasters, terrorism, war and telecommunication and electrical failures. Furthermore, we have little or no control over the security measures and computer systems of our third-party service providers. While we and, to our knowledge, our third-party service providers have not experienced any such system failure, accident or security breach to date, if such an event were to occur and cause interruptions in our operations or the operations of our third-party service providers, it could result in a material disruption of our drug development programs. If any disruptions occur, they could have a material adverse effect on our business.
We are subject to legal, regulatory, financial and other risks with our operations outside the U.S.
We operate globally and are attempting to develop products in multiple countries. Consequently, we face complex legal and regulatory requirements in multiple jurisdictions, which may expose us to certain financial and other risks. International operations are subject to a variety of risks, including:
| · | foreign currency exchange rate fluctuations; | |
| · | greater difficulty in overseeing foreign operations; | |
| · | logistical and communications challenges; | |
| · | potential adverse changes in laws and regulatory practices, including export license requirements, trade barriers, tariffs and tax laws; | |
| · | burdens and costs of compliance with a variety of foreign laws; | |
| · | political and economic instability; | |
| · | increases in duties and taxation; | |
| · | foreign tax laws and potential increased costs associated with overlapping tax structures; | |
| · | greater difficulty in protecting intellectual property; | |
| · | the risk of third-party disputes over ownership of intellectual property and infringement of third-party intellectual property by our products; and | |
| · | general social, economic and political conditions in these foreign markets. |
ITEM 1B. UNRESOLVED STAFF COMMENTS
None.
ITEM 2. PROPERTIES
Our principal office is located at 3960 Howard Hughes Parkway, Suite 500, Las Vegas, Nevada 89169 (“Leased Premises”). The office we lease consist of approximately 100 square feet plus the use of certain shared facilities, such as a lobby, conference rooms, a kitchen and open workspaces. The term of the first lease agreement expired on April 30, 2022. On January 13, 2022, we entered into a new lease agreement for the Leased Premises for an additional six-month term, expiring on October 31, 2022.
ITEM 3. LEGAL PROCEEDINGS
There is no material litigation currently pending against us or any of our subsidiaries or to which any of our or our subsidiaries’ property is subject. To our knowledge, there is no material litigation against any of our officers or directors in their capacity as such, and no such litigation is contemplated by any governmental authorities.
ITEM 4. MINE SAFETY DISCLOSURES
Not applicable.
| 83 |
PART II
ITEM 5. MARKET FOR REGISTRANT’S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES.
On August 10, 2021, our shares of common stock commenced trading on the Nasdaq Capital Market (“Nasdaq”). Prior to that, shares of our common stock were quoted on the OTC Link™ quotation platform of OTC Markets Group, Inc. (“OTCQB”) as an Over-The-Counter Bulletin Board company under the classification of OTCQB utilizing the trading symbol “PMCB.” As a result of a 1:1500 reverse stock split effective July 12, 2021, our trading symbol was changed to “PMCBD” until August 6, 2021. Thereafter, it reverted to “PMCB.”
The following table sets forth the post reverse stock split (1:1500) high and low bid quotations reported on the OTCQB through August 9, 2021 and Nasdaq through April 30, 2022 for our shares for each quarter during the two fiscal years (“FYs”) ended April 30, 2022 and 2021. The prices reflect inter-dealer prices, without retail mark-up, mark-down or commission and may not necessarily represent actual transactions.
| Date | Bid Price | |||||||
| FY 2022 | HIGH | LOW | ||||||
| First Quarter | $ | 27.16 | 5.56 | |||||
| Second Quarter | $ | 12.01 | 2.25 | |||||
| Third Quarter | $ | 3.05 | 1.89 | |||||
| Fourth Quarter | $ | 2.51 | 1.79 | |||||
| FY 2021 | ||||||||
| First Quarter | $ | 52.39 | 19.10 | |||||
| Second Quarter | $ | 28.36 | 10.45 | |||||
| Third Quarter | $ | 40.15 | 5.97 | |||||
| Fourth Quarter | $ | 55.22 | 20.90 | |||||
As of April 30, 2022, there were 20,721,047 issued and outstanding shares of our common stock. We are informed these shares are held by approximately 1,400 shareholders of record.
Dividend Policy
We have not paid and do not plan to pay cash dividends now. Our Board will decide any future payment of dividends, depending on the results of operations, financial condition, capital requirements and other relevant factors.
Securities Authorized for Issuance under Equity Compensation Plans
See Item 12 of Part III of this Report regarding information about securities authorized for issuance under our equity compensation plans.
Recent Issuance of Unregistered Securities
We issued Common Stock Purchase Warrants (“Warrants”) to Aeon (defined below) in connection with our Block Trades (defined below). We issued Warrants to purchase the number of shares of our restricted common stock listed below.
| 84 |
The Warrants have a five-year term and represent 5% of the number of shares of common stock sold at an exercise price equal to the price per share at which the shares were sold in the Block Trade. They are exercisable by the holder at any time from the sale date through and including the expiration date set forth in the Warrant. Each Warrant has a specified exercise price as set forth below.
| Sale Date | Warrants Issued | Exercise Price |
| June 13, 2019 | 926 | $13.50 |
| July 15, 2019 | 1,296 | $13.50 |
| August 7, 2019 | 2,333 | $7.50 |
| February 24, 2020 | 667 | $7.50 |
| March 24, 2020 | 2,333 | $7.50 |
| March 31, 2020 | 667 | $7.50 |
| April 7, 2020 | 1,667 | $15.00 |
| April 21, 2020 | 556 | $22.50 |
| July 10, 2020 | 2,733 | $15.00 |
| July 18, 2020 | 2,333 | $11.25 |
| July 19, 2020 | 889 | $11.25 |
| July 27, 2020 | 1,667 | $11.25 |
| August 3, 2020 | 3,000 | $11.25 |
| August 6, 2020 | 2,733 | $15.00 |
| August 6, 2020 | 3,333 | $7.50 |
| August 7, 2020 | 3,667 | $7.50 |
| August 7, 2020 | 1,667 | $11.25 |
| August 10, 2020 | 889 | $11.25 |
| August 23, 2021 | 7,000,000 | $5.00 |
| August 23, 2021 | 1,050,000 | $6.25 |
In addition to issuances of unregistered securities by us to our officers and directors previously disclosed in our Quarterly Reports on Form 10-Q, our Form 8-Ks and this Report, on March 1, 2021, we issued 29,144 shares of restricted common stock relating to the cashless exercise of twenty-six (26) warrant agreements to an investment banker. The non-cash expense for these share issuances was zero.
All such shares were issued without registration under the Securities Act in reliance upon the exemption afforded by Section 4(a)(2) of the Securities Act based on the limited number of investors, the sophistication of the individuals involved and the use of restrictive legends on the share certificates issued to prevent a public distribution of the relevant securities.
ITEM 6. SELECTED FINANCIAL DATA
Reserved.
ITEM 7. MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS
The following discussion may contain forward-looking statements that involve risks and uncertainties. As described under the caption “Cautionary Note Regarding Forward-Looking Statements,” our actual results could differ materially from those discussed here. Factors that could cause or contribute to such differences include, but are not limited to, any factors discussed in this section as well as factors described in Part II, Item 1A. “Risk Factors” and under the caption “Cautionary Note Regarding Forward-Looking Statements.”
Overview
We are a biotechnology company focused on developing and preparing to commercialize cellular therapies for cancer, diabetes and malignant ascites based upon our proprietary cellulose-based live cell encapsulation technology we refer to as Cell-in-a-Box®. We are working to advance clinical research and development of new cellular-based therapies in oncology and diabetes.
| 85 |
We are actively engaged preparing for a Phase 2b clinical trial in LAPC using encapsulated live cells like those used in the previous Phase 1/2 and Phase 2 clinical trials discussed above.
On September 1, 2020, we submitted an IND to the FDA for our planned Phase 2b clinical trial in LAPC. On October 1, 2020, we received notice from the FDA that it had placed our IND on clinical hold. On October 30, 2020, the FDA sent a letter to us setting forth the reasons for the clinical hold and specific guidance on what we must do to have the clinical hold lifted.
For the purpose of addressing the clinical hold, we assembled a team of regulatory and scientific experts to respond to the items requested by the FDA. That team has been working to complete the list of items requested by the FDA. For a complete discussion of what the FDA requires of us and the efforts we have undertaken to lift the clinical hold, see Item 1. Business under the Section entitled, “Clinical Hold” of this Report.
We are also developing a way to delay the production and accumulation of malignant ascites that results from many types of abdominal cancerous tumors. Our therapy for malignant ascites involves using the same encapsulated cells we employ for pancreatic cancer but placing the encapsulated cells in the peritoneal cavity of a patient and administering ifosfamide intravenously.
In addition to these cancer programs, we have also been considering ways to exploit the benefits of the Cell-in-a-Box® technology to develop therapies for cancer that involve prodrugs based upon certain constituents of the Cannabis plant. However, until the FDA allows us to commence our clinical trial in LAPC and we are able to validate our Cell-in-a-Box® encapsulation technology in a clinical trial, we are not spending any further resources developing our Cannabis Program.
Finally, we have been developing a potential therapy for Type 1 diabetes and insulin-dependent Type 2 diabetes Our product candidate for the treatment of diabetes consists of encapsulated genetically modified insulin-producing cells. The encapsulation will be done using the Cell-in-a-Box® technology. Implanting these encapsulated cells in the body is designed to function as a bio-artificial pancreas for purposes of insulin production.
Reverse Stock Split
Effective July 12, 2021, we filed a Certificate of Change with the Nevada Secretary of State that authorized a 1:1500 reverse stock split of our common stock. The reverse stock split resulted in reducing the authorized number of shares of our common stock from 50 billion to thirty-three million three hundred thirty-three thousand three hundred thirty-four with a par value of $0.0001 per share. Any fractional shares resulting from the reverse stock split were rounded up to the next whole share. All warrants, option, share and per share information in this Report gives retroactive effect to such 1:1500 reverse stock split.
COVID-19 Impact on Our Financial Condition and Results of Operations
COVID-19 continues to cause uncertainty and significant, industry-wide delays in clinical trials. The availability of vaccines holds promise for the future; however, new variants of the virus and potential waning immunity from vaccines may result in continued impact from COVID-19 in the future, which could adversely impact our operations. Although we are not yet in a clinical trial, we have filed an IND with the FDA to commence a clinical trial in LAPC. While the IND has been placed on clinical hold by the FDA, we have assessed the impact of COVID-19 on our operations and that impact is increasing. The impact relates to delays in: (i) completing studies required by the FDA; (ii) manufacturing a new batch of CypCap™ for our planned clinical trial in LAPC; (iii) manufacturing syringes of CypCaps™ for some of the preclinical studies to be completed and use in our Malignant Ascites Program; and (iv) securing third party contractors to conduct various R&D projects. As a result, there may be delays in generating responses to the requests from the FDA related to the clinical hold. Many of these potential delays are also due to the impact of COVID-19 in foreign countries where we are conducting these preclinical studies, including India, Europe, Singapore and Thailand. There have also been supply chain interruptions
due to COVID-19.
| 86 |
As a result of COVID-19 and the mitigation efforts to address it, we may experience additional disruptions that could adversely impact our business and clinical trial, if allowed to proceed, including: (i) delays or difficulties in enrolling patients in our Phase 2b clinical trial if the FDA allows us to go forward with the trial; (ii) delays or difficulties in clinical site activation, including difficulties in recruiting clinical site investigators and clinical site personnel; (iii) delays in clinical sites receiving the supplies and materials needed to conduct our clinical trial, including interruption in global shipping that may affect the transport of our clinical trial product; (iv) changes in local regulations as part of a response to COVID-19 which may require us to change the ways in which our clinical trial is to be conducted, which may result in unexpected costs, or to discontinue the clinical trial altogether; (v) diversion of healthcare resources away from the conduct of clinical trials, including the diversion of hospitals serving as our clinical trial sites and hospital staff supporting the conduct of our clinical trial; (vi) interruption of key clinical trial activities, such as clinical trial site monitoring, due to limitations on travel imposed or recommended by federal or state governments, employers and others, or interruption of clinical trial subject visits and study procedures, the occurrence of which could affect the integrity of clinical trial data; (vii) risk that participants enrolled in our clinical trials will acquire COVID-19 while the clinical trial is ongoing, which could impact the results of the clinical trial, including by increasing the number of observed adverse events; (viii) delays in necessary interactions with local regulators, ethics committees, and other important agencies and contractors due to limitations in employee resources or forced furlough of government employees; (ix) limitations in employee resources that would otherwise be focused on the conduct of our clinical trial because of sickness of employees or their families or the desire of employees to avoid contact with large groups of people; (x) refusal of the FDA to accept data from clinical trials in affected geographies; and (xi) interruption or delays to our clinical trial activities.
As a result of COVID-19, commencement of our planned clinical trial to treat LAPC may be delayed beyond the lifting of the clinical hold by the FDA should that occur. Also, enrollment may be difficult for the reasons discussed above. In addition, after enrollment in the trial, if patients contract COVID-19 during their participation in the trial or are subject to isolation or shelter in place restrictions, this may cause them to drop out of our clinical trial, miss scheduled therapy appointments or follow-up visits or otherwise fail to follow the clinical trial protocol. If patients are unable to follow the clinical trial protocol or if the trial results are otherwise affected by the consequences of COVID-19 on patient participation or actions taken to mitigate COVID-19 spread, the integrity of data from the clinical trial may be compromised or not be accepted by the FDA. This could further adversely impact or delay our clinical development program if the FDA allows it to proceed.
Clinical trials in the biopharma industry may be delayed due to COVID-19. There are numerous reasons for these potential delays. For example, patients have shown a reluctance to enroll or continue in a clinical trial due to fear of exposure to COVID-19 when they are in a hospital or doctor’s office. There are local, regional and state-wide orders and regulations restricting usual normal activity by people. These discourage and interfere with patient visits to a doctor’s office if the visit is not COVID-19 related. Healthcare providers and health systems have shifted their resources away from clinical trials toward the care of COVID-19 patients. The FDA and other healthcare providers are making product candidates for the treatment of COVID-19 a priority over product candidates unrelated to COVID-19.
It is highly speculative in projecting the effects of COVID-19 on our proposed clinical development program and the Company generally. Moreover, the various precautionary measures taken by many governmental authorities around the world in order to limit the spread of COVID-19 has had and may continue to have an adverse effect on the global markets and global economy, including on the availability and pricing of employees, resources, materials, manufacturing and delivery efforts and other aspects of the global economy. The continuation of the COVID-19 pandemic could materially disrupt our business and operations, hamper our ability to raise additional funds or sell or securities, continue to slow down the overall economy, curtail consumer spending, interrupt our sources of supply, and make it hard to adequately staff our operations. The effects of COVID-19 quickly and dramatically change over time. Its evolution is difficult to predict, and no one is able to say with certainty when the pandemic will fully cease to have an impact on our operations.
Performance Indicators
Non-financial performance indicators used by management to manage and assess how the business is progressing will include, but are not limited to, the ability to: (i) acquire appropriate funding for all aspects of our operations; (ii) acquire and complete necessary contracts; (iii) complete activities for producing genetically modified human cells and having them encapsulated for our preclinical studies and the planned Phase 2b clinical trial in LAPC; (iv) have regulatory work completed to enable studies and trials to be submitted to regulatory agencies; (v) complete all required tests and studies on the cells and capsules we plan to use in our clinical trial in patients with LAPC; (vi) ensure completion of the production of encapsulated cells according to cGMP regulations to use in our planned clinical trial; (vii) complete all of the tasked the FDA requires of us in order to have the clinical hold lifted; and (viii) obtain approval from the FDA to lift the clinical hold on our IND that we may commence our planned Phase 2b clinical trial in LAPC.
| 87 |
There are numerous items required to be completed successfully to ensure our final product candidate is ready for use in our planned clinical trial in LAPC. The effects of material transactions with related parties, and certain other parties to the extent necessary for such an undertaking, may have substantial effects on both the timeliness and success of our current and prospective financial position and operating results. Nonetheless, we are actively working to ensure strong ties and interactions to minimize the inherent risks regarding success. We do not believe there are factors which will cause materially different amounts to be reported than those presented in this Report. We aim to assess this regularly to provide accurate information to our shareholders.
Liquidity and Capital Resources
As of April 30, 2022, our cash and cash equivalents totaled approximately $85.4 million, compared to approximately $2.2 million as of April 30, 2021. Working capital was approximately $84.8 million as of April 30, 2022, and approximately $1.6 million as of April 30, 2021. The increase in cash is attributable to proceeds from the sale of our common stock net of an increase in our operating expenses.
On August 9, 2021, the Company entered into an underwriting agreement to offer and sell shares of common stock, pre-funded warrants to purchase common stock and warrants to purchase common stock in a public offering (“First Offering”). The gross proceeds of the First Offering were $15 million, before deduction of underwriting discounts, commissions, and estimated offering expenses.
In August 2021, the Company received twenty-seven (27) cash exercise notices relating to the common warrants with respect to the First Offering totaling 2,522,387 warrant shares (“Warrant Exercises”). The Company received approximately $10,720,000 and issued 2,522,387 shares of common stock as a result of the exercise notices.
On August 19, 2021, the Company entered into a securities purchase agreement (“Securities Purchase Agreement”) with certain institutional investors (“Purchasers”) pursuant to which the Company agreed to sell in a registered direct offering (“Registered Direct Offering”), shares of the Company’s common stock and pre-funded warrants to purchase shares of common stock. Further, pursuant to the Securities Purchase Agreement, in a concurrent private placement (together with the Registered Direct Offering, “Second Offering”), the Company also agreed to issue to the Purchasers unregistered warrants (“Series A Warrants”) to purchase shares of common stock. The Company received gross proceeds from the Second Offering, before deducting placement agent fees and other estimated offering expenses payable by the Company, of approximately $70 million. On November 17, 2021, the Company’s Registration Statement on Form S-3 registering the resale of the common stock underlying the Series A Warrants was declared effective by the U.S. Securities and Exchange Commission (“Commission”).
During the year ended April 30, 2022, funding in the amount of approximately $87.4 million was provided by investors to maintain and expand our operations and R&D through the First Offering and the Second Offering and the Warrant Exercises. Sales of our common stock, pre-funded warrants and exercise of Common Warrants occurred in the First Offering, Second Offering, and the Warrant Exercises.
During the year ended April 30, 2021, the Company sold and issued approximately 462,000 shares of common stock, pursuant to an effective S-3 registration statement, at prices ranging from approximately $15 to $45 per share. Net of underwriting discounts, legal, accounting, and other offering expenses, the Company received proceeds of approximately $4.7 million from the sale of these shares for the year ended April 30, 2021.
On May 14, 2018, we entered into amendments to all of the material agreements with SG Austria and Austrianova. See Section entitled, History of the Business” in Item 1. Business. above for a description of these amendments. We have no other off-balance sheet arrangements that could have a material current effect or that are reasonably likely to have a material adverse effect on our financial condition, changes in financial condition, revenues or expenses, results of operations, liquidity, capital expenditures or capital resources.
Year ended April 30, 2022, compared to year ended April 30, 2021
Revenue
We had no revenues in the fiscal years ended April 30, 2022, and 2021.
| 88 |
Operating Expenses
The total operating expenses during the year ended April 30, 2022, increased by $769,033 to $4,392,014 from $3,622,981 in the year ended April 30, 2021. The increase is mainly attributable to increases in compensation expense, legal and professional expense, and consulting expense in 2022 from 2021, net of decreases in R&D costs and director fees.
| Operating expenses: | Year ended April 30, 2022 | Change - Increase (Decrease) and Percent | Year ended April 30, 2021 | |||||||||
| R&D | $ | 690,937 | $ | (225,312 | ) | $ | 916,249 | |||||
| (25% | ) | |||||||||||
| Compensation expense | $ | 1,544,751 | $ | 115,601 | $ | 1,429,150 | ||||||
| 8% | ||||||||||||
| Director fees | $ | 256,490 | $ | (16,740 | ) | $ | 273,230 | |||||
| (6% | ) | |||||||||||
| General and administrative, legal and professional | $ | 1,899,836 | $ | 895,484 | $ | 1,004,352 | ||||||
| 89% | ||||||||||||
Loss from Operations
Loss from operations during the year ended April 30, 2022, increased by $769,033 to $4,392,014 from $3,622,981 in the year ended April 30, 2021. The increase is mainly attributable to increases in compensation expense, legal and professional expense, and consulting expense in 2022 from 2021, net of decreases in R&D costs and director fees.
Other Income (Expenses), Net
Other income, net for the year ended April 30, 2022, was $152,853 as compared to other expense, net of $71,745 in the year ended April 30, 2021. Other income, net for the year ended April 30, 2022, is attributable to interest income of $157,645 net of interest expense and other expenses of $4,792. Other income, net for the year ended April 30, 2021, is attributable to the forgiveness of the Paycheck Protection Program loan and accrued interest of $75,979 net of interest and other expenses of $4,234.
Discussion of Operating, Investing and Financing Activities
The following table presents a summary of our sources and uses of cash for the years ended April 30, 2022, and 2021.
| Year Ended April 30, 2022 | Year Ended April 30, 2021 | |||||||
| Net cash used in operating activities: | $ | (4,117,319 | ) | $ | (3,330,889 | ) | ||
| Net cash used in investing activities: | $ | – | $ | – | ||||
| Net cash provided by financing activities: | $ | 87,311,244 | $ | 4,636,807 | ||||
| Effect of currency rate exchange | $ | 4,625 | $ | 1,327 | ||||
| Increase in cash | $ | 83,198,550 | $ | 1,307,245 | ||||
Operating Activities:
The cash used in operating activities for the years ended April 30, 2022, and 2021, is a result of our net losses offset by securities issued for services and compensation, changes to prepaid expenses, accounts payable and accrued expenses.
| 89 |
Investing Activities: We had no investing activities for the years ended April 30, 2022, and 2021.
Financing Activities:
The cash provided from financing activities for the years ended April 30, 2022, and 2021, is mainly attributable to the proceeds from the sale of our common stock.
Critical Accounting Estimates and Policies
Our Consolidated Financial Statements are prepared in accordance with U.S. generally accepted accounting principles (“U.S. GAAP”). We are required to make assumptions and estimates about future events and apply judgments that affect the reported amounts of assets, liabilities, revenue and expenses and the related disclosures. We base our assumptions, estimates and judgments on historical experience, current trends and other factors that management believes to be relevant at the time our Consolidated Financial Statements are prepared. On a regular basis, management reviews the accounting policies, assumptions, estimates and judgments to ensure that our Consolidated Financial Statements are presented fairly and in accordance with U.S. GAAP. However, because future events and their effects cannot be determined with certainty, actual results could differ from our assumptions and estimates, and such differences could be material.
Our significant accounting policies are discussed in Note 2 of the Notes to our Consolidated Financial Statements included in Item 8, “Financial Statements and Supplementary Data” of this Report. Management believes that the following accounting estimates are the most critical to aid in fully understanding and evaluating our reported financial results and require management’s most difficult, subjective or complex judgments resulting from the need to make estimates about the effects of matters that are inherently uncertain. Management has reviewed these critical accounting estimates and related disclosures with our Board.
Research and Development Expenses
R&D expenses consist of costs incurred for direct and overhead-related research expenses and are expensed as incurred. Costs to acquire technologies, including licenses, which are utilized in R&D and that have no alternative future use are expensed when incurred. Technology developed for use in our product candidates is expensed as incurred until technological feasibility has been established.
Stock-Based Compensation
Our stock-based compensation plans are described in Note 4 and 5 of the Notes of the Consolidated Financial Statements to this Report. We follow the provisions of ASC 718, Compensation - Stock Compensation (“ASC 718”), which requires the measurement and recognition of compensation expense for all stock-based awards made to employees.
Net Income (Loss) Per Share
Basic net income (loss) per share of common stock is computed using the weighted-average number of shares of common stock outstanding. Diluted net income (loss) per share of common stock is computed using the weighted-average number of shares of common stock and shares of common stock equivalents outstanding. Potentially dilutive stock options and warrants to purchase 10,813,635 and 44,314 post reverse stock split shares of common stock at April 30, 2022, and 2021, respectively, were excluded from the computation of diluted net income (loss) per share because the effect would be anti-dilutive.
New Accounting Pronouncements
For a discussion of all recently adopted and recently issued but not yet adopted accounting pronouncements, see “Recent Accounting Pronouncements” in Note 2 of our Notes to our Consolidated Financial Statements included in Item 8, “Financial Statements and Supplementary Data” of this Report.
| 90 |
ITEM 7A. QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK
We are a smaller reporting company and are not required to include information called for by this Item 7A.
ITEM 8. FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA
Our Consolidated Balance Sheets, as of April 30, 2022, and 2021, and our Consolidated Statements of Operations, Comprehensive Loss, Stockholders Equity and Cash Flows for each of the two years in the period ended April 30, 2022, and associated Notes and Schedules, together with the reports thereon of our independent registered public accounting firm, are set forth on pages F-1 to F-27 of this Report and are incorporated by reference herein.
ITEM 9. CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURES
Our principal independent public accountant is Armanino LLP (“Armanino”). During our fiscal years ended April 30, 2022, and 2021, there have been no disagreements with Armanino on any matter of accounting principles or practices, financial statement disclosure or auditing scope or procedure which, if not resolved to Armanino’s satisfaction, would have caused Armanino to refer to the subject matter in its report on our Consolidated Financial Statements for such periods.
During our fiscal years ended April 30, 2022, and 2021, there were no “reportable events” requiring disclosure pursuant to Item 304(a)(1)(v) of Regulation S-K. As used herein, the term “reportable event” means any of the items listed in paragraphs (a)(1)(v)(A) - (D) of Item 304 of Regulation S-K.
ITEM 9A. CONTROLS AND PROCEDURES
Evaluation of Disclosure Controls and Procedures
Our Chief Executive Officer, President and General Counsel, as our principal executive officer (“Chief Executive Officer”), and our Chief Financial Officer, as our principal financial officer (“Chief Financial Officer”), evaluated the effectiveness of our “disclosure controls and procedures,” as such term is defined in Rule 13a-15(e) promulgated under the Exchange Act. Disclosure controls and procedures are designed to ensure that the information required to be disclosed in the reports that we file or submit to the Commission pursuant to the Exchange Act are recorded, processed, summarized and reported within the period specified by the Commission’s rules and forms and are accumulated and communicated to our management, including our Chief Executive Officer, as appropriate to allow timely decisions regarding required disclosures. Based upon this evaluation, our Chief Executive Officer and our Chief Financial Officer have concluded that, as of April 30, 2022, that certain of our disclosure controls and procedures were not effective due to the material weaknesses in internal control over financial reporting. This is described below in Management’s Report on Internal Control over Financial Reporting.
A control system, no matter how well conceived and operated, can provide only reasonable, not absolute, assurance that the objectives of the control system are met. Further, the design of a control system must reflect the fact that there are resource constraints, and the benefits of controls must be considered relative to their costs. Because of the inherent limitations in all control systems, no evaluation of controls can provide absolute assurance that all control issues and instances of fraud, if any, within the Company have been detected. These inherent limitations include the realities that judgments in decision-making can be faulty and that breakdowns can occur because of simple error or mistake. Also, controls can be circumvented by the individual acts of some persons, by collusion of two or more people or by management override of the controls. The design of any system of controls is also based in part upon certain assumptions about the likelihood of future events. There can be no assurance that any design will succeed in achieving its stated goals under all potential future conditions.
Management’s Report on Internal Controls over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal controls over financial reporting as that term is defined in Exchange Act Rules 13a-15(f) and 15d-15(f). Our internal controls over financial reporting are designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with U.S. GAAP.
| 91 |
A material weakness is a deficiency, or a combination of deficiencies, in internal controls over financial reporting such that there is a reasonable possibility that a material misstatement of our annual or interim financial statements will not be prevented or detected in a timely basis.
Under the supervision and with the participation of our Chief Executive Officer and our Chief Financial Officer, management conducted an evaluation of the effectiveness of our internal controls over financial reporting as of April 30, 2022, based on the criteria outlined in Internal Control-Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (“COSO”) and identified the following material weaknesses in internal controls over financial reporting:
| · | Insufficient Segregation of Duties of the Chief Financial Officer. We have delegated some of the duties of our Chief Financial Officer to other personnel within the Company and have added review and approval processes performed by the Chief Executive Officer. However, we have determined that we still have insufficient segregation of the duties of our Chief Financial Officer. We plan to hire an additional person to work for our Chief Financial Officer to enable sufficient segregation of his duties. |
Because of this material weakness, our Chief Executive Officer and our Chief Financial Officer concluded that, as of April 30, 2022, our internal controls over financial reporting were not effective based on the COSO criteria.
We plan to make changes to our procedures and controls that we believe are reasonably likely to strengthen and materially affect our internal controls over financial reporting. The one material weakness should be eliminated during fiscal year 2023.
Prior to the remediation of our material weakness, there remains risk that the processes and procedures on which we currently rely will fail to be sufficiently effective, which could result in material misstatement of our financial position or results of operations and require a restatement. Because of the inherent limitations in all control systems, no evaluation of controls - even where we conclude the controls are operating effectively - can provide absolute assurance that all control issues, including instances of fraud, if any, have been detected. These inherent limitations include the realities that judgments in decision making can be faulty, and breakdowns can occur because of simple error or mistake. Additionally, controls can be circumvented by the individual acts of a person, by collusion of two or more people, or by management override of the controls. The design of any system of controls also is based in part upon certain assumptions about the likelihood of future events; accordingly, there can be no assurance that any design will succeed in achieving its stated goals under all potential future conditions. Over time, our control systems, as we develop them, may become inadequate because of changes in conditions or the degree of compliance with the policies or procedures may deteriorate. Because of the inherent limitations in a cost-effective control system, misstatements due to error or fraud may occur and not be detected and could be material to our financial statements.
Remediation of a Material Weakness
Throughout the year ended April 30, 2022, we undertook remediation measures related to a previously reported material weakness in internal control over financial reporting. The previously reported material weakness related to insufficient information technology controls and documentation. We completed the remediation measures during the year ended April 30, 2022, including testing of the design and implementation of the related controls. We acquired and installed an accounting software package to record our transactions to provide the level of controls required by COSO. Based on these procedures, we believe that this previously reported material weakness has been remediated.
Changes in Internal Controls over Financial Reporting
Other than described above in this Item 9A, there were no changes to our internal control over financial reporting during the fiscal year ended April 30, 2022, that have materially affected, or are reasonably likely to materially affect, our internal controls over financial reporting.
The Certifications of our Principal Executive and Principal Financial Officer required in accordance with Rule 13a-14(a) under the Exchange Act and Section 302 of the Sarbanes-Oxley Act of 2002 (“Certifications”) are attached to this Report. The disclosures set forth in this Item 9A contain information concerning: (i) the evaluation of our disclosure controls and procedures, and changes in internal control over financial reporting, referred to in paragraph 4 of the Certifications; and (ii) material weaknesses in the design or operation of our internal control over financial reporting, referred to in paragraph 5 of the Certifications. The Certifications should be read in conjunction with this Item 9A for a more complete understanding of the matters covered by the Certifications.
| 92 |
ITEM 9B. OTHER INFORMATION
On May 8, 2022, we entered into amendments to the employment agreements with each of Kenneth L. Waggoner, our Chief Executive Officer and President, and Carlos A. Trujillo, our Chief Financial Officer. The terms of such amended employment agreements are summarized in Part III, Item 11. “Executive Compensation—Employment Arrangements” of this Report, which summaries are qualified in their entirety by reference to the full text of such amended employment agreements filed herewith as Exhibits 10.40 and 10.41.
ITEM 9C. DISCLOSURE REGARDING FOREIGN JURISDICTIONS THAT PREVENT INSPECTIONS
Not applicable.
| 93 |
PART III
ITEM 10. DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE
As of July 15, 2022, our directors and executive officers are:
| Age | Position | |
| Kenneth L. Waggoner | 74 | Chairman of the Board, Chief Executive Officer, President and General Counsel |
| Gerald W. Crabtree | 81 | Director and Chief Scientific Officer |
| Carlos A. Trujillo | 64 | Director and Chief Financial Officer |
| Thomas Liquard | 49 | Director |
| Michael M. Abecassis | 64 | Director |
| Raymond C.F. Tong | 63 | Director |
| Matthias Löhr | 63 | Director |
Kenneth L. Waggoner
Kenneth L. Waggoner became our Chief Executive Officer and President in November 2013. Shortly thereafter, Mr. Waggoner assumed the additional position of General Counsel. In April 2014, Mr. Waggoner became a full-time employee as the Chief Executive Officer, President and General Counsel of both PharmaCyte and Viridis Biotech, a wholly owned subsidiary of PharmaCyte. Mr. Waggoner has been a member of the Board since September 2014. Mr. Waggoner has over forty-five years of experience in management, business, operations and the practice of law. It was his education, training, experience and leadership skills that led us to elect him to the Board and appoint him Chairman.
Mr. Waggoner began his professional career as an attorney in private practice. From 1986 to 2003, he was a senior partner with the international law firm Brobeck, Phleger and Harrison (“Brobeck”). He was the Managing Partner of Brobeck’s Los Angeles office. While at Brobeck, Mr. Waggoner served as a member of the Executive Committee and Policy Committee. Mr. Waggoner was the co-Chairman of Brobeck’s worldwide Environmental Law Group.
Mr. Waggoner’s career included leadership and legal positions with Fortune 100 companies most of his professional career. From 2003 to 2005, Mr. Waggoner served as the Vice President and General Counsel of Chevron’s global downstream operations where he was responsible for the overall management of legal services to the North American, Latin American, European and Asian Products Companies. While at Chevron, Mr. Waggoner led the restructuring of Chevron’s global Legal Department following Chevron’s acquisition of Texaco.
From 2005 until September 2013, Mr. Waggoner was the principal of the Law Offices of Kenneth L. Waggoner & Associates. During that time, he held leadership and legal positions with several start-up companies and provided legal counsel and business advice to his clients.
Mr. Waggoner received his Juris Doctorate with honors from Loyola University School of Law in Los Angeles in 1973.
Gerald W. Crabtree
Gerald W. Crabtree is our Chief Scientific Officer and has been a member of the Board since February 2013. He has served as Chief Scientific Officer since October 14, 2020. Prior to that, Dr. Crabtree was our Chief Operating Officer. Given the major importance to developing treatments for cancer and diabetes coupled with Dr. Crabtree’s education, training and experience, Dr. Crabtree was appointed to the Board.
Dr. Crabtree’s background in the biomedical sciences has been substantial, having been involved with various biopharmaceutical companies where he has alternatively supervised and coordinated the development of multiple drug candidates, prepared clinical protocols, investigator brochures, monographs, and research and review articles.
| 94 |
Dr. Crabtree has over 50 years of experience in the biomedical sciences sector with the majority of that being in the cancer area. Dr. Crabtree served as the Director of Project Planning and Management (Oncology and Immunology) at Bristol-Myers Squibb (“BMS”) from 1990 to 1997. While at BMS, Dr. Crabtree established and directed the department that coordinated the development of all oncologic and immunologic drugs from initial discovery through regulatory approval. He also served as Project Manager for the development of the major anticancer agent, Taxol. Taxol ultimately became a multi-billion-dollar drug for BMS and is still widely used to treat a variety of cancers. From 1985 to 1990, Dr. Crabtree was the Director of Pharmacology at Viratek, a subsidiary of ICN Pharmaceuticals, in Costa Mesa, California, where he worked on the development of anticancer drugs first developed at the Nucleic Acid Research Institute, a joint venture between Eastman Kodak and ICN Pharmaceuticals. He also helped coordinate the development of ribavirin, Viratek's landmark antiviral drug. From 1970 through 1985, Dr. Crabtree was a member of the faculty of Brown University where he was involved in both basic and clinical cancer research.
Dr. Crabtree received his Ph.D. in Biochemistry from the University of Alberta, Edmonton, Alberta, Canada, and has published over 80 articles in peer-reviewed journals. He was a National Cancer Institute of Canada Research Fellow, is currently a member of the American Society of Clinical Oncology and was a member of the American Association for Cancer Research from the early 1990s until recently and has served on research grant review committees for the National Institutes of Health and the American Cancer Society.
Carlos A. Trujillo
Carlos A. Trujillo has been our Chief Financial Officer and a member of the Board since March 2017. He began working for us as an independent contractor in September 2014. In January 2015, Mr. Trujillo became a full-time employee as the Vice President of Finance of both us and Viridis Biotech, and in March 2017, Mr. Trujillo was appointed as our Chief Financial Officer. Mr. Trujillo has over three decades of experience in management, business, operations and financial accounting. It was his education, experience and leadership skills that led us to elect him to the Board.
Mr. Trujillo is a Certified Public Accountant with an active license from the State of California. He has more than three decades of experience in finance, accounting and management. Mr. Trujillo started his career in public accounting and was the manager of an audit department a large regional public accounting firm. Mr. Trujillo then established a consulting and accounting practice which he operated for ten years and provided services as the Chief Financial Accountant to numerous organizations in several different industries. His experience has extended to companies in the biotechnology, telecommunications, manufacturing, construction and real estate development sectors.
For the last fourteen years, Mr. Trujillo has been the Chief Financial Officer for both privately held and publicly traded and multinational companies. From June 2008 through September 2014, Mr. Trujillo was the Chief Financial Officer of VelaTel Global Communications, Inc. As a result, he brings experience to us in preparing and filing periodic reports with the Commission, in mergers and acquisitions and in the filing of comprehensive financial statements.
Mr. Trujillo received his Bachelor of Accounting degree from California State University, Fullerton in 1982.
Thomas Liquard
Thomas Liquard has been a member of the Board since April 2015. Mr. Liquard has more than 15 years of experience in the pharmaceutical industry, having held various commercialization, product development and leadership roles with large pharmaceutical and biotechnology companies.
Mr. Liquard currently serves as the Senior Vice President of Product Development at Neurelis, Inc., a San Diego based biotechnology company. He joined Neurelis in late 2017. He From August 2015 to August 2017, Mr. Liquard was the Chief Executive Officer of Immuron, a Melbourne, Australia-based pharmaceutical company. Prior to Immuron, Mr. Liquard served as the Chief Executive Officer and Chief Operating Officer of Alchemia, a major Australian pharmaceutical company. Mr. Liquard worked for Alchemia from October 2013 to November 2014. Mr. Liquard spent the previous seven years with Pfizer, Inc. based in New York, where he held various senior commercial positions. His last was as Senior Director, Portfolio Development Leader and Emerging Markets for the Established Products portfolio. In that role, Mr. Liquard drove business development (M&A, licensing, partnerships) and internal product development initiatives.
| 95 |
Mr. Liquard was appointed to the Board because of his experience and expertise in leading positions with life science-based biotech and pharmaceutical companies. We believed that his seven-year tenure with Pfizer, one of the world’s leading pharmaceutical companies, where he played leading roles in the development of that company’s portfolio development, was a needed asset to us. Mr. Liquard received his Master of Business Administration in Finance and Strategy from the Columbia Business School and a Bachelor of Science degree from the University of Southern California.
Michael M. Abecassis
Michael M. Abecassis, MD was appointed to the Board in July 2017. Since November 2019, Dr. Abecassis has been Dean of the University of Arizona College of Medicine – Tucson. Prior to that and since 1992, Dr. Abecassis was a transplantation surgeon at the Northwestern University Feinberg School of Medicine. Dr. Abecassis was appointed to the Board because of his demonstrated leadership qualities in academia, in the clinic and throughout his career in medicine. These attributes and his experience in the medical field translate directly to the work being undertaken by us in the cancer arena and have led us to elect him to the Board.
Dr. Abecassis was the Director of the Comprehensive Transplant Center of the Feinberg School of Medicine. He was also the Chief of Transplant Surgery in the Department of Surgery at Feinberg and a James Roscoe Miller Distinguished Professor of Medicine at Feinberg.
Dr. Abecassis received his Medical Degree from the University of Toronto in 1983 and was awarded a Master of Business Administration degree from the Kellogg School of Management at Northwestern University in 2000. After his postgraduate tenure in Toronto, Dr. Abecassis began his clinical career as Assistant Professor of Surgery and Director of Liver Transplantation and Hepatobiliary Surgery at the University of Iowa. In 1993, Dr. Abecassis became Northwestern University’s Director of Liver Transplantation, where he initiated Northwestern’s liver transplant program. In 2004, Dr. Abecassis was named Chief of the Division of Transplantation at the Feinberg School of Medicine. He became Founding Director of the Comprehensive Transplant Center at Northwestern in 2009 and was appointed Dean for Clinical Affairs at the Feinberg School of Medicine in 2008, serving until 2011.
Dr. Abecassis has received continuous funding from the National Institutes of Health (“NIH”) for the past 17 years. He is the principal investigator in research that includes both laboratory and clinical studies. He is also the principal investigator of the clinical core of the NIH Genomics of Transplantation Cooperative Research Program. Dr. Abecassis has trained numerous clinical and research fellows.
Dr. Abecassis is a member of the Society of University Surgeons and the American Surgical Association and was President of the American Society of Transplant Surgeons 2010-2011. He has served and continues to serve on the Editorial Boards of major scientific journals (Hepatology, Surgery, Transplantation and Liver Transplantation) and is a reviewer for all major journals related to surgery and transplantation. He has served as a member of NIH grant study sections and special emphasis panels relating to both transplantation and virology. He is a permanent member of the National Institute of Allergy and Infectious Diseases study section for career development and training grants.
Dr. Abecassis has been a course director for the American Society of Transplant Surgeons Leadership Development Program since 2010 and was course director for the Advanced Leader Development Program in 2013 at Northwestern’s Kellogg School of Management. He was a voting member of the Medicare Coverage Advisory Committee and served on the United HealthCare Group Physician Advisory Board on Healthcare Performance and Quality. Dr. Abecassis has been a member of various local, regional and national regulatory committees and has published seminal papers on both the regulatory and financial aspects of transplantation, including the Healthcare Reform and the Affordable Care Act.
Raymond C.K Tong
Raymond C.K. Tong, MD serves as Chief Executive Officer of Harmony Medical Inc., an Asian investment group active in the introduction and distribution of medical and healthcare products and services in China and throughout Asia. He is also Chairman of the Business Development Committee of Shanghai Kedu Healthcare Group, the largest medical equipment third-party service provider in China, representing products from GE, Philips, Siemens, Kodak and other multi-nationals as well as local companies. He was appointed to the Board in October 2017. It was his stellar career in the medical field, as well as his significant connections to the investment community throughout Asia, leadership skills and business acumen and experience that caused us to elect him to the Board.
| 96 |
Dr. Tong has been a Director of Medifocus Inc. since January 27, 2015. He was also a Director of Shanghai CP Guojian Pharmaceutical, one of the first and largest bio-pharmaceutical manufacturers in China. In addition, Dr. Tong is the founding Director and Chief Executive Officer of VetCell Therapeutics Asia, a cell therapy company focused on providing cell-based treatments for use in veterinary medicine in Asia.
Dr. Tong’s earlier career includes senior management positions in China with Pfizer and Ball Corporation. He was also responsible for the Healthcare Investment Division of CITIC in Hong Kong. CITIC is the largest conglomerate in China and an established global player, with businesses covering healthcare, financial services, resources, energy, manufacturing, engineering and many others.
Dr. Tong received his medical degree from the University of Toronto in Ontario, Canada in 1983. He also received a Ph.D. degree in neurophysiology and an M.B.A. degree. After receiving his medical degree, Dr. Tong founded a chain of medical clinics in the Province of Ontario where he served as Medical Director and Chief Physician. During this period, he also served as a consultant and an investigator in several clinical trials. In 1989, Dr. Tong returned to Hong Kong, where he was born and resided before medical school, and spent the next 19 years in prominent corporate appointments with several multinational medical and pharmaceutical companies discussed above.
Matthias Löhr
Matthias Löhr, MD was appointed to the Board in March 2022. Dr. Löhr is a licensed physician, board-certified internist and Professor of Gastroenterology and Hepatology at the Karolinska Institute of Stockholm, Sweden. He leads the pancreatic team at Karolinska University Hospital. He has served as Professor of Molecular Gastroenterology at the University of Heidelberg with a same-named unit at the German Cancer Research Center in Heidelberg Germany. He has worked as a translational scientist and principal investigator in clinical studies in gastrointestinal oncology for many years. In addition to being highly published, he has extensive scientific and grant review experience, and has received multiple awards and distinctions. These attributes and his experience in the medical field translate directly to the work being undertaken by us in the cancer arena have led us to elect him to the Board.
Dr. Löhr served as the Principal Investigator for the Phase 1/2 and Phase 2 clinical trials of the PharmaCyte’s pancreatic cancer therapy that were completed in the early 2000s. He is familiar with the Cell-in-a-Box® live-cell encapsulation technology that forms the core of our pancreatic cancer therapy. He also administered our therapy for pancreatic cancer in clinical trials in patients with advanced, inoperable pancreatic cancer.
Dr. Löhr has also previously served as a consultant to us in connection with our development of treatments for pancreatic cancer and diabetes using the Cell-in-a-Box® technology. He has expertise in both diseases and has a thorough understanding of our technology and its use in a clinical setting.
In 2000, Dr. Löhr was appointed Professor of Molecular Gastroenterology at the University of Heidelberg and became Head of the Division at the German Cancer Research Center, which he led until 2010. Dr. Löhr has authored more than 340 original peer-reviewed scientific papers and more than 50 reviews. He has authored six books. He has been granted six patents and is an Editor Board Member of the Journal of Clinical Medicine, Pancreatology, Scientific Reports, and the World Journal of Gastroenterology.
Dr. Löhr holds MD and PhD degrees from the Universities of Hamburg and Rostock. Following receipt of his medical degree, he served a residency in pathology in Hamburg, Germany, and residencies in internal medicine and gastroenterology, where he became chief resident and later attending physician and assistant professor at the University of Rostock.
Family Relationships
There are no family relationships among our executive officers, directors and significant employees.
Legal Proceedings
As of April 30, 2022, our personnel do not have any involvement in legal proceedings requiring disclosure pursuant to the rules and regulations of the Commission.
| 97 |
Code of Ethics
Our Board has adopted a written Code of Business Conduct and Ethics, an Insider Trading Policy and Software Policies that apply to our directors, officers, employees and contractors. These documents can be viewed and downloaded from the “Governance” dropdown menu of our website under the “Company” tab. The content of these documents is not incorporated into this Form 10-K.
Corporate Governance and Committees
Board Leadership and Structure
The Chairman of the Board presides at all meetings of the Board. Mr. Waggoner serves as the Chairman of the Board and as our Chief Executive Officer, President and General Counsel.
The Board does not have a policy on whether or not the roles of Chief Executive Officer and Chairman of the Board should be separate. The Board believes that it should be free to make a choice from time to time in any manner that is in the best interests of the Company and our stockholders.
Audit Committee
The Audit Committee is currently comprised of Dr. Michael Abecassis, Dr. Tong, and Mr. Liquard. The Chairman of the Audit Committee is Mr. Liquard. The primary purposes of our Audit Committee are to assist the Board in fulfilling its legal and fiduciary obligations with respect to matters involving the accounting, auditing, financial reporting, internal control, legal compliance and risk management functions of the Company, including, assisting the Board’s oversight of: (i) the integrity of our financial statements; (ii) the effectiveness of our internal control over financial reporting; (iii) our compliance with legal and regulatory requirements; (iv) the qualifications and independence of our independent registered public accounting firm; and (v) the performance of our internal audit function and independent registered public accounting firm.
Our Board has determined that each member of our Audit Committee is independent within the meaning of the rules of Nasdaq. Our Board has determined that the Chairman of the Audit Committee, Mr. Liquard, is an “audit committee financial expert,” as that term is defined in Item 407(d) of Regulation S-K under the Exchange Act.
Our Audit Committee charter can be viewed and downloaded from the “Governance” dropdown menu of our website under the “Company” tab.
Compensation Committee
The Compensation Committee is currently comprised of Mr. Liquard, Dr. Tong and Dr. Löhr. The Chairperson of the Compensation Committee is Dr. Tong. The primary purposes of our Compensation Committee are: (i) to establish and maintain our executive compensation policies and compensation consistent with corporate objectives and stockholder interests; (ii) to oversee the competency and qualifications of our senior management personnel and the provisions of senior management succession planning; and (iii) to advise the Board with respect to director compensation issues.
The Compensation Committee, which is composed of independent directors, provides overall guidance for our executive compensation policies and determines the value and elements of compensation for our executive officers.
Our Compensation Committee charter can be viewed and downloaded from the “Governance” dropdown menu of our website under the “Company” tab.
Nominating and Corporate Governance Committee
The Nominating and Corporate Governance Committee is currently comprised of Dr. Abecassis and Dr. Tong. The Chairperson of the Nominating and Corporate Governance Committee is Dr. Abecassis.
| 98 |
The primary purposes of the Nominating Committee are: (i) to recommend to the Board the nomination of individuals who are qualified to serve as our directors and on committees of the Board; (ii) to advise the Board with respect to the composition, size, structure and procedures of the Board; (iii) to advise the Board with respect to the composition, size and membership of the Board’s committees; (iv) to advise the Board with respect to corporate governance principles applicable to the Company; and (v) to oversee the evaluation of the Board as a whole and the evaluation of its individual members standing for re-election. The Nominating Committee also has responsibility for reviewing and approving all transactions that are “related party” transactions under the Commission’s rules.
The Nominating Committee does not set specific, minimum qualifications that nominees for director must meet in order for the Nominating Committee to recommend them to the Board, but rather believes that each nominee should be evaluated based on his or her individual merits, considering our needs and the composition of the Board. Members of the Nominating Committee discuss and evaluate possible candidates in detail and suggest individuals to explore in more depth. Once a candidate is identified whom the Nominating Committee wants to seriously consider and move toward nomination, the Chairman of the Nominating Committee enters into a discussion with that nominee candidate. Subsequently, the Chairperson will discuss the qualifications of the candidate with the other members of the Nominating Committee, and the Nominating Committee will then make a final recommendation with respect to that candidate to the Board.
Board Practices
Our business and affairs are managed under the direction of our Board. The primary responsibilities of our Board are to provide oversight, strategic guidance, counseling and direction to our senior management.
Policy Regarding Board Attendance
Our directors are expected to attend meetings of the Board as frequently as necessary to properly discharge their responsibilities and to spend the time needed to prepare for each such meeting. If an annual meeting of stockholders is held, our directors are expected to attend that meeting, but we do not have a formal policy requiring them to do so.
Shareholder Communications
We have a process for shareholders who wish to communicate with our Board. Shareholders who wish to communicate with our Board may write to the Board at our address set forth at the beginning of this Report. These communications will be reviewed by our Chief Executive Officer and Chief Financial Officer. They will determine whether the communications should be presented to our Board. The purpose of this screening is to allow the Board to avoid having to consider irrelevant or inappropriate communications.
ITEM 11. EXECUTIVE COMPENSATION
This section discusses the material components of the executive compensation program for our executive officers who are named in the “Summary Compensation Table” below (each a “Named Executive Officer”), as well as the director compensation program for our directors. As a smaller reporting company, we are not required to include a Compensation Discussion and Analysis and have elected to comply with the scaled disclosure requirements applicable to smaller reporting companies.
For our fiscal year ended April 30, 2022, our Named Executive Officers and their positions were as follows:
| · | Kenneth L. Waggoner, Chief Executive Officer, President, General Counsel and Chairman of the Board; |
| · | Gerald W. Crabtree, Chief Scientific Officer and Director; and |
| · | Carlos A. Trujillo, Chief Financial Officer and Director. |
The following tables provide information about compensation earned during our fiscal years ended April 30, 2022, and 2021, by our Named Executive Officers.
| 99 |
Summary Compensation Table
| Name | Principal Position | Fiscal Year | Salary ($) | Stock Awards ($)(1) | Option Awards ($)(1) | Total ($) | ||||||||||||||
| Kenneth L. Waggoner (2) | Chief Executive Officer, | 2022 | $ | 886,344 | $ | 18,080 | $ | 14,727 | $ | 919,151 | ||||||||||
| President and | 2021 | $ | 433,333 | $ | 105,960 | $ | 77,212 | $ | 616,505 | |||||||||||
| General Counsel | ||||||||||||||||||||
| Gerald W. Crabtree, (2) | Chief Scientific Officer | 2022 | $ | 128,827 | $ | 3,013 | $ | 4,909 | $ | 136,749 | ||||||||||
| 2021 | $ | 94,333 | $ | 17,660 | $ | 25,738 | $ | 137,731 | ||||||||||||
| Carlos A. Trujillo (2) | Chief Financial Officer | 2022 | $ | 609,979 | $ | 12,053 | $ | 9,819 | $ | 631,851 | ||||||||||
| 2021 | $ | 300,000 | $ | 70,640 | $ | 51,474 | $ | 422,114 | ||||||||||||
(1) The amounts in the columns titled “Stock Awards” and “Option Awards” reflect the grant date fair values of awards made during the identified fiscal year, as computed in accordance with FASB ASC Topic 718 and the assumptions stated in Note 4 and Note 5 of the Consolidated Financial Statements to this Report.
(2) We did not pay or accrue any other compensation, in the form of bonuses, incentive plan compensation or nonqualified deferred compensation earnings to any Named Executive officer for services as an executive officer during the fiscal years ended April 30, 2022, and 2021; neither were there any perquisites or other personal benefits payable to our Named Executive Officers.
Outstanding Equity Awards at Fiscal Year End
| Option Awards | Stock Awards |
| Name | Number of Securities Underlying Unexercised Options (#) Exercisable (1) | Number of Securities Underlying Unexercised Options (#) Unexercisable | Option Exercise Price ($) | Option Expiration Date | Number of Shares or Units of Stock That Have Not Vested (#)(1) | Market Value of Shares or Units of Stock That Have Not Vested ($)(2) | |||||||||||||||||
| Kenneth L. Waggoner | |||||||||||||||||||||||
| 3,000 | – | $ | 81.00 | 12/31/2023 | – | $ | – | ||||||||||||||||
| 3,000 | – | $ | 74.25 | 03/20/2024 | – | $ | – | ||||||||||||||||
| 3,000 | - | $ | 61.20 | 01/02/2025 | – | $ | – | ||||||||||||||||
| 3,000 | - | $ | 10.05 | 12/31/2025 | – | $ | – | ||||||||||||||||
| 1,000 | 2,000 | $ | 2.50 | 01/01/2027 | – | $ | – | ||||||||||||||||
| – | – | $ | – | – | 1,600 | $ | 3,728 | ||||||||||||||||
| Gerald W. Crabtree | |||||||||||||||||||||||
| 1,000 | – | $ | 81.00 | 12/31/2023 | – | $ | – | ||||||||||||||||
| 1,000 | – | $ | 74.25 | 12/31/2024 | – | $ | – | ||||||||||||||||
| 1,000 | – | $ | 61.20 | 01/02/2025 | – | $ | – | ||||||||||||||||
| 1,000 | – | $ | 10.05 | 12/31/2026 | – | $ | – | ||||||||||||||||
| 334 | 667 | $ | 2.50 | 01/01/2027 |
– | $ | – | ||||||||||||||||
| – | – | $ | – | – | 267 | $ | 622 | ||||||||||||||||
| Carlos A. Trujillo | |||||||||||||||||||||||
| 2,000 | – | $ | 81.00 | 12/31/2023 | – | $ | – | ||||||||||||||||
| 2,000 | – | $ | 74.25 | 12/31/2024 | – | $ | – | ||||||||||||||||
| 2,000 | – | $ | 61.20 | 01/02/2025 | – | $ | – | ||||||||||||||||
| 2,000 | – | $ | 10.05 | 12/31/2025 | – | $ | – | ||||||||||||||||
| 667 | 1,334 | $ | 2.50 | 01/0/2027 | – | $ | – | ||||||||||||||||
| – | – | $ | – | – | 1,067 | $ | 2,486 | ||||||||||||||||
_______________________
| (1) | Subject to the Named Executive Officer’s continued employment, 1/12th of each grant vests monthly after the grant date. The unexercisable/unvested awards shown in this table were each granted effective as of January 1, 2022. |
| (2) | The market value is based on the closing stock price of $2.33 on April 30, 2022, the last day of trading in this fiscal year. |
| 100 |
Employment Arrangements
Kenneth L. Waggoner
We have entered into an Amended and Restated Executive Compensation Agreement with Mr. Waggoner (“Waggoner Compensation Agreement”) with an effective date of January 1, 2022. The current term of the Waggoner Compensation Agreement extends until December 31, 2024, with annual extensions at the end of the term (or any extension of the term), unless we or Mr. Waggoner provide 90-days written notice of termination. The Waggoner Compensation Agreement provides that Mr. Waggoner will serve as a member of our Board, as our Chief Executive Officer, President and General Counsel and as the Chief Executive Officer and General Counsel of our subsidiary Viridis Biotech, Inc. Under this agreement, Mr. Waggoner is paid a base salary of $520,000 subject to annual increases in the discretion of our Compensation Committee and shall be eligible to receive cash incentive compensation (“Bonus”). Mr. Waggoner is eligible to participate in the Company’s 2021 Equity Incentive Plan (“2021 Plan”). On May 20, 2022, the Compensation Committee granted Mr. Waggoner (i) a stock option grant to purchase 529,000 shares of common stock exercisable over a ten-year term at an exercise price per share equal to the closing price of the common stock on the date of grant, vesting at the rate of 25% immediately and the remaining vesting monthly over three years from the date of grant, approximately 11,000 option shares per month, and (ii) a grant of 150,800 restricted stock units, vesting at the rate of 25% immediately and an additional 25% on each anniversary of the grant date.
If Mr. Waggoner’s employment is terminated by us without “Cause” or by him for “Good Reason” (as such terms are defined in the Waggoner Compensation Agreement), then subject to his execution of a timely release, he is entitled to: (i) severance equal to two times the sum of his base salary at the time his employment terminates, (ii) payment of the annual bonus, if any, earned by Mr. Waggoner for the year preceding the year of termination, or, if greater, the target bonus, if any, for the year of termination, (iii) accelerated vesting of any unvested stock or option awards and (iv) continued health coverage for Mr. Waggoner and his family and life insurance coverage for Mr. Waggoner, if any, for 18 months at the Company’s expense.
Notwithstanding the foregoing, if Mr. Waggoner’s employment is terminated by us without Cause or by him for Good Reason within two years after a “Change in Control” (as such term is defined in the Waggoner Compensation Agreement) or within six months prior to a Change in Control, then the base salary and bonus, if any, component of severance would be paid in lump sum. Also, Mr. Waggoner would be entitled to receive a full Code Section 280G tax gross-up, with respect to any amounts that may be subject to the excise tax provisions under Code Section 280G.
If Mr. Waggoner’s employment ceases due to his death, (i) any otherwise unvested equity awards held by him at the time of his death would become vested, (ii) his eligible dependents would be entitled to continued healthcare coverage at the Company’s expense for up to 18 months, and (iii) his designated beneficiary or estate would receive the proceeds, if any, from any life insurance.
If Mr. Waggoner’s employment is terminated due to “Disability” (as such term is defined in the Waggoner Compensation Agreement) he would receive continued health coverage and life insurance coverage, if any, for 18 months at our expense, as well as any disability benefits payable under any long-term disability plan or policy we maintain. In addition, any otherwise unvested equity awards would then become vested.
Additionally, Mr. Waggoner is bound by confidentiality and non-disparagement provisions as well as non-solicitation and non-competition covenants that apply during the term of his employment and for twenty-four months after termination of his employment.
Gerald W. Crabtree
We have entered into an Executive Compensation Agreement with Dr. Crabtree (“Crabtree Compensation Agreement”). The current term of the Crabtree Compensation Agreement extends until December 31, 2022 with annual extensions at the end of the term (or any extension of the term) unless we or Dr. Crabtree provide 90-days written notice of termination. The Crabtree Compensation Agreement provides that Dr. Crabtree will serve as a member of our Board, as our Chief Scientific Officer and as the Chief Operating Officer of our subsidiary Viridis Biotech. Dr. Crabtree is paid a base salary of $84,000 subject to annual increases in the discretion of our Compensation Committee. The Crabtree Compensation Agreement also provides that, during his continued employment, Dr. Crabtree will receive annual stock grants of 400 shares of restricted common stock, vesting at the rate of 33 shares per month, and an annual stock option grant to purchase 1,000 shares of common stock exercisable over a five-year term at an exercise price per share equal to the closing price of the common stock on the date of grant, vesting at the rate of 83 option shares per month.
All other terms regarding severance benefits, treatment on a change in control, employment termination due to death/disability and restrictive covenants are substantially the same as disclosed above for the Waggoner Agreement.
| 101 |
Carlos A. Trujillo
We have entered into an Amended and Restated Executive Compensation Agreement with Mr. Trujillo (“Trujillo Compensation Agreement”) with an effective date of January 1, 2022. The current term of the Trujillo Compensation Agreement extends until December 31, 2024, with annual extensions at the end of the term (or any extension of the term) unless we or Mr. Trujillo provide 90-days written notice of termination.
The Trujillo Compensation Agreement provides that Mr. Trujillo will serve as a member of our Board and as our Chief Financial Officer. Mr. Trujillo is paid an annual base salary of $380,000, subject to annual increases at the discretion of the Compensation Committee and shall be eligible to receive an annual Bonus. Mr. Trujillo is eligible to participate in the 2021 Plan. On May 20, 2022, the Compensation Committee granted Mr. Trujillo (i) a stock option grant to purchase 201,860 shares of common stock exercisable over a ten-year term at an exercise price per share equal to the closing price of the common stock on the date of grant, vesting at the rate of 25% immediately and the remaining vesting monthly over three years from the date of grant, approximately 4,200 option shares per month, and (ii) a grant of 57,540 restricted stock units, vesting at the rate of 25% immediately and an additional 25% on each anniversary of the grant date.
All other terms regarding severance benefits, treatment on a change in control, employment termination due to death/disability and restrictive covenants are substantially the same as disclosed above for the Waggoner Agreement.
Directors Compensation
The following table sets forth information concerning compensation paid or to our directors, other than our Named Executive Officers who also serve as directors, during the year ended April 30, 2022.
Director Compensation Table
| Name | Fees Earned ($) | Stock Awards ($)(1) | Option Awards ($)(1)(2) | Total ($) | ||||||||||||
| Thomas Liquard | $ | 50,000 | 8,868 | 5,551 | $ | 64,419 | ||||||||||
| Thomas C.K Yuen | $ | 50,000 | 8,868 | 5,551 | $ | 64,419 | ||||||||||
| Michael M. Abecassis | $ | 50,000 | 5,411 | 3,456 | $ | 58,867 | ||||||||||
| Raymond C.K. Tong | $ | 50,000 | 1,065 | 798 | $ | 51,863 | ||||||||||
| Matthias Löhr | $ | 12,500 | – | – | $ | 12,500 | ||||||||||
| (1) | The amounts in the columns titled “Stock Awards” and “Option Awards” reflect the grant date fair values of awards made during the fiscal year ended April 30, 2022, as computed in accordance with FASB ASC Topic 718 and the assumptions stated in Note 4 and Note 5 of the Consolidated Financial Statements to this Report. |
| (2) | As of April 30, 2022, the non-employee directors held unexercised options to purchase shares as follows: Mr. Liquard, 1,503, Dr. Abecassis, 2,470 and Dr. Tong, 1,670 shares. These include options granted during the year ended April 30, 2022 (shown in this column) and options granted in prior years. |
Each non-employee director is party to an agreement to serve as a director. The agreements provide that each non-employee director receives a cash retainer of $12,500 per quarter (pro-rated for periods of service less than a quarter). In addition, we annually grant to each non-employee director: (i) 334 shares of our common stock; and (ii) a stock option to purchase 334 shares of our common stock with a term of five years and an exercise price per share equal to the closing price of the common stock on the date of grant. Each of these equity awards is fully vested upon grant.
Our three employee directors (who are also Named Executive Officers) do not receive additional compensation for their service on the Board. For information regarding the compensation of our three employee directors, please see above, under the heading “Executive Compensation.”
| 102 |
ITEM 12. SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS
The following table sets forth as of July 15, 2022, certain information with respect to the beneficial ownership of our common stock by each person known by us to be the beneficial owner of more than five percent (5%) of our common stock, by each of our directors, by each of our Named Executive Officers and by all executive officers and directors as a group.
| Name and Address | Amount and Nature of Beneficial Ownership (1) | Percentage of Common Stock (1) | ||||||
| Mitchell P. Kopin | 1,231,482 | (2) | 5.7% | |||||
| Sabby Volatility Warrant Master Fund, Ltd. | 1,260,928 | (3) | 5.8% | |||||
| Iroquois Master Fund Ltd. | 1,309,099 | (4) | 6.1% | |||||
| Kenneth L. Waggoner, Chairman of the Board, Chief Executive Officer, President and General Counsel | 263,052 | (5) | 1.2% | |||||
| Gerald W. Crabtree, Chief Scientific Officer and Board Member | 16,308 | * | ||||||
| Carlos A. Trujillo, Chief Financial Officer and Board Member | 106,028 | (6) | * | |||||
| Thomas Liquard, Board Member | 3,504 | * | ||||||
| Michael M. Abecassis, Board Member | 5,272 | * | ||||||
| Raymond C.K. Tong, Board Member | 3,338 | * | ||||||
| Matthias Löhr, Board Member | 3,338 | * | ||||||
| All directors and executive officers as a group (7 persons) | 400,840 | 1.8% | ||||||
________________________________
* Indicates percentage is less than 1.0%.
| (1) | Percentages based on 21,601,047 shares of common stock issued and outstanding as of July 15, 2022, in addition to the options to purchase shares that are unexercised, but which are exercisable within sixty days of July 15, 2022, which are presented below: |
| (2) | This information is based on a Form 13 G/A filed with the SEC on February 11, 2022 by Mitchell P. Kopin (“Kopin”). Kopin reported sole and shared voting and sole and shared dispositive power of 1,231,482 shares of common stock underlying currently exercisable warrants. The address of Kopin is c/o Intracoastal Capital, LLC, 245 Palm Trail, Delray Beach, Florida 33483. |
| (3) | This information is based on a Form 13 G/A filed with the SEC on January 4, 2022 by Sabby Volatility Warrant Master Fund, Ltd. (“Sabby”). Sabby reported sole and shared voting and sole and shared dispositive power of 1,260,928 shares of common stock underlying currently exercisable warrants. The address of Sabby is c/o Ogier Fiduciary Services (Cayman) Limited, 89 Nexus Way, Camana Bay, Grand Cayman KY1-9007, Cayman Islands. |
| (4) | This information is based on a Form 13 D/A filed with the SEC on July 11, 2022 by Iroquois Master Fund Ltd. (“Iroquois”). Iroquois reported sole and shared voting and sole and shared dispositive power of 1,309,099 shares of common stock underlying currently exercisable warrants. The address of Iroquois is 2 Overhill Road, Suite 400, Scarsdale, New York 10583. |
| (5) | Includes 529,000 options and 150,800 restricted stock units contingent upon stockholder approval. |
| (6) | Includes 201,860 options and 57,540 restricted stock units contingent upon stockholder approval. |
Exercisable options within sixty days of July 15, 2022:
| Kenneth L. Waggoner, JD | 240,927 | |||
| Gerald W. Crabtree, PhD | 4,667 | |||
| Carlos A. Trujillo, CPA | 96,211 | |||
| Thomas Liquard | 1,837 | |||
| Michael M. Abecassis, MD | 2,804 | |||
| Raymond C.K. Tong, MD | 1,670 | |||
| Matthias Löhr, MD | 334 |
The address of all beneficial owners is 3960 Howard Hughes Parkway, Suite 500, Las Vegas, Nevada, 89169. Each person has sole voting and investment power with respect to the shares of common stock.
| 103 |
Securities Authorized for Issuance under Equity Compensation Plans
The following table sets forth certain aggregated information with respect to compensation plans (including individual arrangements) under which our securities are authorized for issuance as of April 30, 2022:
| Plan category | Number of securities to be issued upon exercise of outstanding options, warrants and rights | Weighted-average exercise price of outstanding options, warrants and rights | Number of securities remaining available for future issuance under equity compensation plans (excluding securities reflected in column (a)) | |||||||||
| (a) | (b) | (c) | ||||||||||
| Equity compensation plans approved by security holders | – | – | – | |||||||||
| Equity compensation plans not approved by security holders | 40,900 | $ | 50.35 | – | ||||||||
| Total | 40,900 | $ | 50.35 | – | ||||||||
Please see Notes 5 and 6 of the Consolidated Financial Statements to this Report for more information regarding our equity compensation arrangements.
ITEM 13. CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE
We had the following related party transactions during the years ended April 30, 2022 and 2021, respectively.
We own 14.3% of the equity in SG Austria and is reported on the cost method of accounting. SG Austria has two subsidiaries: (i) Austrianova; and (ii) Austrianova Thailand. We purchased products and services from these subsidiaries in the approximate amounts of $323,000 and $405,000 in the years ended April 30, 2022, and 2021, respectively.
In April 2014, we entered a consulting agreement with Vin-de-Bona pursuant to which it agreed to provide professional consulting services to us. Vin-de-Bona is owned by Prof. Günzburg and Dr. Salmons, both of whom are involved in numerous aspects of our scientific endeavors relating to cancer and diabetes (Prof. Gunzburg is the Chairman of Austrianova, and Dr. Salmons is the Chief Executive Officer and President of Austrianova). The term of the agreement is for 12 months, automatically renewable for successive 12-month terms. After the initial term, either party can terminate the agreement by giving the other party 30 days’ written notice before the effective date of termination. The amounts we paid Vin-de-Bona for the years ended April 30, 2022, and 2021, were approximately $114,000 and $82,000, respectively. In addition, during the years ended April 30, 2022, and 2021, we issued 167 and 167 common shares, respectively, to Dr. Salmons. We recorded a noncash consulting expense of approximately $400 and $5,000 relating to these share issuances for the years ended April 30, 2022, and 2021, respectively.
Except for Mr. Liquard, Dr. Abecassis, Dr. Tong and Dr. Löhr, the Board has determined that none of our directors satisfy the definition of Independent Director as established in the Nasdaq Marketplace Rules. Mr. Liquard, Dr. Abecassis, Dr. Tong and Dr. Löhr have been determined by the Board to be Independent Directors.
| 104 |
ITEM 14. PRINCIPAL ACCOUNTANT FEES AND SERVICES
A summary of the fees billed by our independent audit firm, Armanino LP, for professional services rendered for the years ended April 30, 2022, and 2021 is set forth below.
| Service | 2022 | 2021 | ||||||
| Audit Fees | $ | 167,239 | $ | 80,196 | ||||
| Audit-Related Fees | 33,238 | 63,590 | ||||||
| Tax Fees | – | – | ||||||
| All Other Fees | 61,149 | – | ||||||
| Total | $ | 261,626 | $ | 143,786 | ||||
During the years ended April 30, 2022, and 2021, we incurred from Armanino $167,239 and $80,196 in annual audit fees, respectively, and $33,238 and $63,590 in quarterly review fees, respectively. Additional fees relating to capital raises were paid to Armanino in the amounts of $61,149 and $0 during the years ended April 30, 2022, and 2021, respectively.
Our Audit Committee pre-approves all services to be performed by our independent auditor. All the services listed above have been pre-approved by our Audit Committee.
ITEM 15. EXHIBITS
(a) Documents filed as part of this Report:
(1) Financial Statements.
Our Consolidated Financial Statements and associated Notes and Schedules, as of April 30, 2022, and 2021, and for each of the two years in the period ended April 30, 2022, together with the reports thereon of our independent registered public accounting firm, are set forth on pages F-1 to F-27 of this Report.
(2) Financial Statement Schedules.
Schedule II - Valuation and Qualifying Accounts for the Years Ended 2022, and 2021 is incorporated by reference to page F-27 of the financial statements included herewith.
| 105 |
(3) Exhibits.
Except as so indicated below and in Exhibit 32.1, the following exhibits are filed as part of, or incorporated by reference into, the Report. Certain of the agreements filed as exhibits contain representations and warranties made by the parties thereto. The assertions embodied in such representations and warranties are not necessarily assertions of fact, but a mechanism for the parties to allocate risk. Accordingly, investors should not rely on the representations and warranties as characterizations of the actual state of facts or for any other purpose at the time they were made or otherwise.
| Exhibit No. | Description | Location | ||
| 3.1 | Articles of Incorporation of the Company, as amended, dated October 31, 2019 | Incorporated by reference from the Company’s Quarterly Report on Form 10-Q filed with the SEC on March 13, 2020. | ||
| 3.2 | Corporate Bylaws. | Incorporated by reference from the Company’s Registration Statement on Form SB-2 (File No. 333-68008) filed with the SEC on August 20, 2001. | ||
| 3.3 | Amendment No. One to the Bylaws of PharmaCyte Biotech, Inc. | Incorporated by reference from the Company’s Current Report on Form 8-K filed with the SEC on September 25, 2014. | ||
| 3.4 | Amendment No. Two to the Bylaws of PharmaCyte Biotech, Inc. | Incorporated by reference from the Company’s Current Report on Form 8-K filed with the SEC on October 3, 2014. | ||
| 3.5 | Amendment No. Three to Bylaws of PharmaCyte Biotech, Inc. | Incorporated by reference from the Company’s Current Report on Form 8-K filed with the SEC on June 4, 2021. | ||
| 3.6 | Amendment No. Four to Bylaws of PharmaCyte Biotech, Inc. | Incorporated by reference from the Company’s Current Report on Form 8-K filed with the SEC on July 6, 2021. | ||
| 3.7 | Certificate of Amendment to Articles of Incorporation of the Company, dated July 2, 2021 | Incorporated by reference from the Company’s Current Report on Form 8-K filed with the SEC on July 6, 2021. | ||
| 3.8 | Certificate of Change to Articles of Incorporation of the Company, dated July 9, 2021 | Incorporated by reference from the Company’s Current Report on Form 8-K filed with the SEC on July 13, 2021 | ||
| 4.1 | Form of Common Stock Certificate. | Incorporated by reference from the Company’s Registration Statement on Form SB-2 (File No. 333-68008) filed with the SEC on August 20, 2001. | ||
| 4.2 | Description of Securities | Filed herewith. | ||
| 4.3 | Form of Common Warrant | Incorporated by reference from the Company’s Current Report on Form 8-K filed with the SEC on August 12, 2021. | ||
| 4.4 | Form of Pre-funded Warrant | Incorporated by reference from the Company’s Current Report on Form 8-K filed with the SEC on August 12, 2021. | ||
| 4.5 | Form of Underwriter’s Warrant | Incorporated by reference from the Company’s Current Report on Form 8-K filed with the SEC on August 12, 2021. | ||
| 4.6 | Form of Pre-Funded Common Stock Purchase Warrant | Incorporated by reference from the Company’s Current Report on Form 8-K filed with the SEC on August 23, 2021. | ||
| 4.7 | Form of Series A Warrant Common Stock Purchase Warrant | Incorporated by reference from the Company’s Current Report on Form 8-K filed with the SEC on August 23, 2021. | ||
| 4.8 | Form of Placement Agent Common Stock Purchase Warrant | Incorporated by reference from the Company’s Current Report on Form 8-K filed with the SEC on August 23, 2021. | ||
| 10.1 | Asset Purchase Agreement, dated May 26, 2011, between SG Austria Pte. Ltd. and the Company. | Incorporated by reference from the Company’s Current Report on Form 8-K filed with the SEC on June 28, 2012. | ||
| 10.2 | First Addendum, dated June 11, 2011, to Asset Purchase Agreement between SG Austria Pte. Ltd. and the Company. | Incorporated by reference from the Company’s Current Report on Form 8-K filed with the SEC on June 28, 2012. | ||
| 10.3 | Second Addendum, dated June 14, 2012, to Asset Purchase Agreement between SG Austria Pte. Ltd. and the Company. | Incorporated by reference from the Company’s Current Report on Form 8-K filed with the SEC on June 28, 2012. | ||
| 10.4 | Third Addendum, dated June 25, 2013, to Asset Purchase Agreement between SG Austria Private Limited and the Company. | Incorporated by reference from the Company’s Current Report on Form 8-K filed with the SEC on July 18, 2013. | ||
| 10.5 | Licensing Agreement, dated June 25, 2013, between Austrianova Singapore Pte. Ltd. and the Company. | Incorporated by reference from the Company’s Current Report on Form 8-K filed with the SEC on July 18, 2013. |
| 106 |
| 10.6 | Manufacturing Framework Agreement, dated March 20, 2014, between Austrianova Singapore Pte. Ltd. and the Company. | Incorporated by reference from the Company’s Annual Report on Form 10-K filed with the SEC on August 4, 2014. | ||
| 10.7 | Master Services Agreement, dated April 7, 2014, between ViruSure GmbH and the Company. | Incorporated by reference from the Company’s Annual Report on Form 10-K filed with the SEC on August 4, 2014. | ||
| 10.8 | Consulting Agreement, dated April 1, 2014, between Vin-de-Bona Trading Company Pte. Ltd. and the Company. | Incorporated by reference from the Company’s Annual Report on Form 10-K filed with the SEC on August 4, 2014. | ||
| 10.9 | License Agreement, dated October 13, 2014, between University of Technology, Sydney and PharmaCyte Biotech Australia Pty Ltd (formerly, Nuvilex Australia Pty Ltd). | Incorporated by reference from Amendment No. 1 to the Company’s Annual Report on Form 10-K/A filed with the SEC on October 17, 2014. | ||
| 10.10 | Master Services Agreement, dated March 7, 2014, between ViruSure GmbH and the Company. | Incorporated by reference from Amendment No. 1 to the Company’s Annual Report on Form 10-K/A filed with the SEC on October 17, 2014. | ||
| 10.11 | Licensing Agreement, dated December 1, 2014, between Austrianova Singapore Pte. Ltd. and the Company. | Incorporated by reference to the Company’s Quarterly Report on Form 10-Q filed with the SEC on December 15, 2014. | ||
| 10.12† | First Stock Option Agreement, dated March 10, 2015, between Kenneth L. Waggoner and the Company. | Incorporated by reference from the Company’s Quarterly Report on Form 10-Q filed with the SEC on March 13, 2015. | ||
| 10.13† | Second Stock Option Agreement, dated March 10, 2015, between Kenneth L. Waggoner and the Company. | Incorporated by reference from the Company’s Quarterly Report on Form 10-Q filed with the SEC on March 13, 2015. | ||
| 10.14† | Executive Compensation Agreement, dated January 1, 2015, between Gerald W. Crabtree and the Company. | Incorporated by reference from the Company’s Quarterly Report on Form 10-Q filed with the SEC on March 13, 2015. | ||
| 10.15† | First Stock Option Agreement, dated March 10, 2015, between Gerald W. Crabtree and the Company. | Incorporated by reference from the Company’s Quarterly Report on Form 10-Q filed with the SEC on March 13, 2015. | ||
| 10.16† | Second Stock Option Agreement, dated March 10, 2015, between Gerald W. Crabtree and the Company. | Incorporated by reference from the Company’s Quarterly Report on Form 10-Q filed with the SEC on March 13, 2015. | ||
| 10.17† | Letter agreement, dated April 20, 2015, between Thomas Liquard and the Company. | Incorporated by reference from the Company’s Current Report on Form 8-K filed with the SEC on April 29, 2015. | ||
| 10.18† | Amendment No. 1, dated December 30, 2015, to Executive Compensation Agreement between Gerald W. Crabtree and the Company. | Incorporated by reference from the Company’s Quarterly Report on Form 10-Q filed with the SEC on March 8, 2016. | ||
| 10.19† | Third Stock Option Agreement, dated December 30, 2015, between Gerald W. Crabtree and the Company. | Incorporated by reference from the Company’s Quarterly Report on Form 10-Q filed with the SEC on March 8, 2016. | ||
| 10.20† | Third Stock Option Agreement, dated December 30, 2015, between Kenneth L. Waggoner and the Company. | Incorporated by reference from the Company’s Quarterly Report on Form 10-Q filed with the SEC on March 8, 2016. | ||
| 10.21 | First Amendment, dated June 30, 2015, to Licensing Agreement, dated December 1, 2014, between Austrianova Singapore Pte. Ltd. and the Company. | Incorporated by reference from the Company’s Annual Report on Form 10-K filed with the SEC on July 29, 2016. | ||
| 10.22 | Second Amendment, dated October 19, 2015, to Licensing Agreement, dated December 1, 2014, between Austrianova Singapore Pte. Ltd. and the Company. | Incorporated by reference from the Company’s Annual Report on Form 10-K filed with the SEC on July 29, 2016. |
| 107 |
| 108 |
| 14.1 | PharmaCyte Biotech, Inc. Code of Business Conduct and Ethics. | Incorporated by reference from the Company’s Current Report on Form 8-K filed with the SEC on September 25, 2014. | ||
| 21.1 | List of Subsidiaries. | Filed herewith. | ||
| 23.1 | Consent of Armanino LLP. | Filed herewith. | ||
| 31.1 | Certification of Chief Executive Officer (Principal Executive Officer) pursuant to Rules 13a-14(a) and 15d-14(a) promulgated under Sarbanes-Oxley Act of 1934, as amended. | Filed herewith. | ||
| 31.2 | Certification of Chief Financial Officer (Principal Financial and Principal Accounting Officer) pursuant to Rules 13a-14(a) and 15d-14(a) promulgated under Sarbanes-Oxley Act of 1934, as amended. | Filed herewith. | ||
| 32.1 | Certification of Chief Executive Officer (Principal Executive Officer) pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002. | Furnished herewith. | ||
| 32.2 | Certification of Chief Financial Officer (Principal Financial and Principal Accounting Officer) pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002. | Furnished herewith. | ||
| 101.INS | Inline XBRL Instance Document - the instance document does not appear in the Interactive Data File because its XBRL tags are embedded within the Inline XBRL document. | Filed herewith. | ||
| 101.SCH | Inline XBRL Taxonomy Extension Schema Document | Filed herewith. | ||
| 101.CAL | Inline XBRL Taxonomy Extension Calculation Linkbase Document | Filed herewith. | ||
| 101.DEF | Inline XBRL Taxonomy Extension Definition Linkbase Document | Filed herewith. | ||
| 101.LAB | Inline XBRL Taxonomy Extension Label Linkbase Document | Filed herewith. | ||
| 101.PRE | Inline XBRL Taxonomy Extension Presentation Linkbase Document | Filed herewith. | ||
| 104 | Cover Page Interactive Data File (formatted as Inline XBRL and contained in Exhibits 101) | Filed herewith. |
† A contract, compensatory plan or arrangement to which a director or executive officer is a party or in which one or more directors or executive officers are eligible to participate.
Financial Statements Schedule:
The following financial statement schedule is set forth on page F-27 of this Report:
Schedule II — Valuation and Qualifying Accounts for the years ended April 30, 2022, and 2021.
All other schedules are omitted because they are not required, not applicable or the information is provided in the financial statements or notes thereto.
ITEM 16. FORM 10-K SUMMARY
None.
| 109 |
SIGNATURES
Pursuant to the requirements of the Securities Exchange Act the registrant has duly caused this report to be signed on its behalf by the undersigned thereunto duly authorized.
| PharmaCyte Biotech, Inc. | |
| July 28, 2022 | By: /s/ Kenneth L. Waggoner |
|
Kenneth L. Waggoner Chief Executive Officer | |
| (Duly Authorized Officer and Principal Executive Officer) | |
| July 28, 2022 |
By: /s/ Carlos A Trujillo Carlos A. Trujillo Chief Financial Officer (Duly Authorized Officer and Principal Financial and Accounting Officer) |
Pursuant to the requirements of the Exchange Act, this Report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
| July 28, 2022 | By: /s/ Kenneth L. Waggoner Kenneth L. Waggoner Chief Executive Officer, Chairman of the Board and Director (Principal Executive Officer) |
| July 28, 2022 | By: /s/ Carlos A. Trujillo Carlos A. Trujillo Chief Financial Officer and Director (Principal Financial and Accounting Officer) |
| July 28, 2022 | By: /s/ Gerald W. Crabtree Gerald W. Crabtree, Director |
| July 28, 2022 | By: /s/ Thomas Liquard Thomas Liquard, Director |
| July 28, 2022 | By: /s/ Michael M. Abecassis |
| Michael M. Abecassis, Director | |
| July 28, 2022 | By: /s/ Raymond C.F. Tong |
| Raymond C.F. Tong, Director | |
| July 28, 2022 | By: /s/ Matthias Löhr |
| Matthias Löhr, Director |
| 110 |
SUPPLEMENTAL INFORMATION TO BE FURNISHED WITH REPORTS
FILED PURSUANT TO SECTION 15(d) OF THE ACT BY REGISTRANTS WHICH HAVE NOT REGISTERED SECURITIES PURSUANT TO SECTION 12 OF THE ACT
The registrant has not sent to its security holders any annual report covering the registrant’s fiscal year ended April 30, 2022.
| 111 |
PHARMACYTE BIOTECH, INC.
FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA
CONTENTS
| F-1 |
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Board of Directors and Stockholders
PharmaCyte Biotech, Inc.
Las Vegas, Nevada
Opinion on the Consolidated Financial Statements
We have audited the accompanying consolidated balance sheets of PharmaCyte Biotech, Inc. and subsidiaries (collectively the "Company") as of April 30, 2022 and 2021, and the related consolidated statements of operations, comprehensive loss, stockholders' equity, and cash flows for each of the two years in the period ended April 30, 2022, and the related notes (collectively referred to as the consolidated financial statements).
In our opinion, the consolidated financial statements present fairly, in all material respects, the consolidated financial position of the Company as of April 30, 2022 and 2021, and the related consolidated results of its operations and cash flows for each of the two years in the period ended April 30, 2022, in conformity with U.S. generally accepted accounting principles. In addition, in our opinion, the consolidated financial statement schedules listed in the accompanying index presents fairly, in all material respects, the information set form therein when read in conjunction with the related consolidated financial statements.
Basis for Opinion
The Company's management is responsible for these consolidated financial statements and consolidated financial statement schedules. Our responsibility is to express an opinion on the Company's consolidated financial statements and on the consolidated financial statement schedules based on our audits. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) (PCAOB) and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the consolidated financial statements and consolidated financial statement schedules are free of material misstatement, whether due to error or fraud. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. As part of our audits we are required to obtain an understanding of internal control over financial reporting but not for the purpose of expressing an opinion on the effectiveness of the Company's internal control over financial reporting. Accordingly, we express no such opinion.
Our audits included performing procedures to assess the risks of material misstatement of the consolidated financial statements and consolidated financial statement schedules, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the consolidated financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the consolidated financial statements. We believe that our audits provide a reasonable basis for our opinion.
Critical Audit Matters
Critical audit matters are matters arising from the current period audit of the consolidated financial statements that were communicated or required to be communicated to the audit committee that (1) relate to accounts or disclosures that are material to the consolidated financial statements and (2) involved our especially challenging, subjective or complex judgments. We determined that there were no critical audit matters.
/s/
July 28, 2022
We have served as the Company's auditor since 2015.
| F-2 |
PHARMACYTE BIOTECH, INC.
CONSOLIDATED BALANCE SHEETS
| April 30, | ||||||||
| 2022 | 2021 | |||||||
| ASSETS | ||||||||
| Current assets: | ||||||||
| Cash and cash equivalents | $ | $ | ||||||
| Prepaid expenses and other current assets | ||||||||
| Total current assets | ||||||||
| Other assets: | ||||||||
| Intangible assets | ||||||||
| Investment in SG Austria | ||||||||
| Other assets | ||||||||
| Total other assets | ||||||||
| Total Assets | $ | $ | ||||||
| LIABILITIES AND STOCKHOLDERS' EQUITY | ||||||||
| Current liabilities: | ||||||||
| Accounts payable | $ | $ | ||||||
| Accrued expenses | ||||||||
| Total current liabilities | ||||||||
| Total Liabilities | ||||||||
| Commitments and Contingencies (Notes 7 and 9) | ||||||||
| Stockholders' equity: | ||||||||
| Common stock, authorized: shares, $ par value; 20,721,047 and shares issued and outstanding as of April 30, 2022, and 2021, respectively | ||||||||
| Additional paid-in capital | ||||||||
| Accumulated deficit | ( | ) | ( | ) | ||||
| Accumulated other comprehensive loss | ( | ) | ( | ) | ||||
| Total stockholders' equity | ||||||||
| Total Liabilities and Stockholders' Equity | $ | $ | ||||||
The accompanying notes are an integral part of these consolidated financial statements.
| F-3 |
PHARMACYTE BIOTECH, INC.
CONSOLIDATED STATEMENTS OF OPERATIONS
| Years Ended April 30, | ||||||||
| 2022 | 2021 | |||||||
| Revenue | $ | $ | ||||||
| Operating expenses: | ||||||||
| Research and development costs | ||||||||
| Compensation expense | ||||||||
| Director fees | ||||||||
| Legal and professional | ||||||||
| General and administrative | ||||||||
| Total operating expenses | ||||||||
| Loss from operations | ( | ) | ( | ) | ||||
| Other income (expense): | ||||||||
| Gain on forgiveness of Paycheck Protection Program loan | ||||||||
| Interest income | ||||||||
| Interest expense | ( | ) | ( | ) | ||||
| Other expense, net | ( | ) | ( | ) | ||||
| Total other income, net | ||||||||
| Net loss | $ | ( | ) | $ | ( | ) | ||
| Basic loss per share | $ | ( | ) | $ | ( | ) | ||
| Diluted loss per share | $ | ( | ) | $ | ( | ) | ||
| Weighted average shares outstanding basic | ||||||||
| Weighted average shares outstanding diluted | ||||||||
The accompanying notes are an integral part of these consolidated financial statements.
| F-4 |
PHARMACYTE BIOTECH, INC.
CONSOLIDATED STATEMENTS OF COMPREHENSIVE LOSS
| Years Ended April 30, | ||||||||
| 2022 | 2021 | |||||||
| Net loss | $ | ( | ) | $ | ( | ) | ||
| Other comprehensive income: | ||||||||
| Foreign currency translation adjustments | ||||||||
| Other comprehensive income | ||||||||
| Comprehensive loss | $ | ( | ) | $ | ( | ) | ||
The accompanying notes are an integral part of these consolidated financial statements.
| F-5 |
PHARMACYTE BIOTECH, INC.
CONSOLIDATED STATEMENTS OF STOCKHOLDERS' EQUITY
YEARS ENDED APRIL 30, 2022, AND 2021
| Common Stock | Additional Paid-in | Accumulated | Accumulated Other Comprehensive | Total Stockholders’ | ||||||||||||||||||||
| Shares | Amount | Capital | Deficit | Loss | Equity | |||||||||||||||||||
| Balance, April 30, 2020 | $ | $ | $ | ( | ) | $ | ( | ) | $ | |||||||||||||||
| Stock issued for compensation | ||||||||||||||||||||||||
| Stock issued for services | ||||||||||||||||||||||||
| Stock issued for cash, net of issuance
costs of $ | ||||||||||||||||||||||||
| Stock issued for warrant exercises | ( | ) | ||||||||||||||||||||||
| Stock-based compensation - options | – | |||||||||||||||||||||||
| Foreign currency translation adjustments | – | |||||||||||||||||||||||
| Net loss | – | ( | ) | ( | ||||||||||||||||||||
| Balance, April 30, 2021 | $ | $ | $ | ( | ) | $ | ( | ) | $ | |||||||||||||||
| Stock issued for compensation | ||||||||||||||||||||||||
| Stock issued for services | ||||||||||||||||||||||||
| Stock issued for cash, net of cash
issuance costs of $ | ||||||||||||||||||||||||
| Stock-based compensation - options | – | |||||||||||||||||||||||
| Issuance of pre-funded warrants | – | |||||||||||||||||||||||
| Reverse stock split adjustment | ( | ) | ||||||||||||||||||||||
| Foreign currency translation adjustments | – | |||||||||||||||||||||||
| Net loss | – | ( | ) | ( | ) | |||||||||||||||||||
| Balance, April 30, 2022 | $ | $ | $ | ( | ) | $ | ( | ) | $ | |||||||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
| F-6 |
PHARMACYTE BIOTECH, INC.
CONSOLIDATED STATEMENTS OF CASH FLOWS
| Years Ended April 30, | ||||||||
| 2022 | 2021 | |||||||
| Cash flows from operating activities: | ||||||||
| Net loss | $ | ( | ) | $ | ( | ) | ||
| Adjustments to reconcile net loss to net cash used in operating activities: | ||||||||
| Gain on forgiveness of Paycheck Protection Program loan | ( | ) | ||||||
| Stock issued for services | ||||||||
| Stock issued for compensation | ||||||||
| Stock-based compensation - options | ||||||||
| Change in operating assets and liabilities: | ||||||||
| Increase (decrease) in prepaid expenses and other current assets | ( | ) | ||||||
| Decrease in other assets | ( | ) | ||||||
| Increase (decrease) in accounts payable | ( | ) | ||||||
| Decrease in accrued expenses | ( | ) | ( | ) | ||||
| Net cash used in operating activities | ( | ) | ( | ) | ||||
| Cash flows from investing activities: | ||||||||
| Net cash used in investing activities | ||||||||
| Cash flows from financing activities: | ||||||||
| Payment of insurance financing loan | ( | ) | ( | ) | ||||
| Proceeds from sale of common stock, net of issuance costs | ||||||||
| Net cash provided by financing activities | ||||||||
| Effect of currency rate exchange on cash and cash equivalents | ||||||||
| Net increase in cash and cash equivalents | ||||||||
| Cash and cash equivalents at beginning of the year | ||||||||
| Cash and cash equivalents at end of the year | $ | $ | ||||||
| Supplemental disclosure of cash flows information: | ||||||||
| Cash paid during the years for income taxes | $ | $ | ||||||
| Cash paid during the years for interest expense | $ | |||||||
| Non-cash equity issuance costs | $ | $ | ||||||
The accompanying notes are an integral part of these consolidated financial statements.
| F-7 |
PHARMACYTE BIOTECH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
NOTE 1 – NATURE OF BUSINESS
PharmaCyte Biotech, Inc. (“Company”) is a biotechnology company focused on developing cellular therapies for cancer, diabetes and malignant ascites based upon a proprietary cellulose-based live cell encapsulation technology known as “Cell-in-a-Box®.” The Cell-in-a-Box® technology is intended to be used as a platform upon which therapies for several types of cancer, including locally advanced, inoperable pancreatic cancer (“LAPC”) will be developed. The current generation of the Company’s product candidate is referred to as “CypCaps™.”
On September 1, 2020, the Company submitted an Investigational New Drug Application (“IND”) to the United States Food and Drug Administration (“FDA”) for a planned Phase 2b clinical trial in LAPC. On October 1, 2020, the Company received notice from the FDA that it had placed the IND on clinical hold. On October 30, 2020, the FDA sent a letter to the Company setting forth the reasons for the clinical hold and specific guidance on what the Company must do to have the clinical hold lifted.
To lift the clinical hold, the FDA has informed the Company that it needs to conduct several additional preclinical studies. The FDA also requested additional information regarding several topics, including DNA sequencing data, manufacturing information and product release specifications. The Company is also in the process of conducting these studies and gathering additional information to submit to the FDA. See “Clinical Hold” below.
The Cell-in-a-Box® encapsulation technology potentially enables genetically engineered live human cells to be used as a means to produce various biologically active molecules. The technology is intended to result in the formation of pinhead sized cellulose-based porous capsules in which genetically modified live human cells can be encapsulated and maintained. In a laboratory setting, this proprietary live cell encapsulation technology has been shown to create a micro-environment in which encapsulated cells survive and flourish. They are protected from environmental challenges, such as the sheer forces associated with bioreactors and passage through catheters and needles. The Company believes that this enables greater cell growth and production of the active molecules. The capsules are largely composed of cellulose (cotton) and are bioinert.
The Company is developing therapies for pancreatic and other solid cancerous tumors by using genetically engineered live human cells that it believes are capable of converting a cancer prodrug into its cancer-killing form. The Company encapsulates those cells using the Cell-in-a-Box® technology and places those capsules in the body as close as possible to the tumor. In this way, the Company believes that when a cancer prodrug is administered to a patient with a particular type of cancer that may be affected by the prodrug the killing of the patient’s cancerous tumor may be optimized.
The Company is also developing a way to delay the production and accumulation of malignant ascites that results from many types of abdominal cancerous tumors. The Company’s therapy for malignant ascites involves using the same encapsulated cells it employs for pancreatic cancer but placing the encapsulated cells in the peritoneal cavity of a patient and administering ifosfamide intravenously.
In addition to the two cancer programs discussed above, the Company has been working on ways to exploit the benefits of the Cell-in-a-Box® technology to develop therapies for cancer that involve prodrugs based upon certain constituents of the Cannabis plant. However, until the FDA allows us to commence our clinical trial in LAPC and we are able to validate our Cell-in-a-Box® encapsulation technology in a clinical trial, we are not spending any further resources developing our Cannabis Program.
Finally, the Company has been developing a potential therapy for Type 1 diabetes and insulin-dependent Type 2 diabetes. The Company’s product candidate for the treatment of diabetes consists of encapsulated genetically modified insulin-producing cells. The encapsulation will be done using the Cell-in-a-Box® technology. Implanting these encapsulated cells in the body is designed to have them function as a bio-artificial pancreas for purposes of insulin production.
| F-8 |
Clinical Hold
On October 1, 2020, we received notice from the FDA that it had placed our IND on clinical hold. On October 30, 2020, the FDA sent us a letter setting forth the reasons for the clinical hold and providing specific guidance on what we must do to have the clinical hold lifted.
In order to address the clinical hold, the FDA has requested that we:
| · | Provide additional sequencing data and genetic stability studies; |
| · | Conduct a stability study on the Company’s final formulated product candidate as well as the cells from the Company’s Master Cell Bank; |
| · | Evaluate the compatibility of the delivery devices (the prefilled syringe and the microcatheter used to implant the CypCaps™) with the Company’s product candidate for pancreatic cancer; |
| · | Provide additional detailed description of the manufacturing process of the Company’s product candidate for pancreatic cancer; |
| · | Provide additional product release specifications for the Company’s encapsulated cells; |
| · | Demonstrate comparability between the 1st and 2nd generation of the Company’s product candidate for pancreatic cancer and ensure adequate and consistent product performance and safety between the two generations; |
| · | Conduct a biocompatibility assessment using the Company’s capsules material; |
| · | Address specified insufficiencies in the Chemistry, Manufacturing and Controls information in the cross-referenced Drug Master File; |
| · | Conduct an additional nonclinical study in a large animal (such as a pig) to assess the safety, activity, and distribution of the product candidate for pancreatic cancer; and |
| · | Revise the Investigators Brochure to include any additional preclinical studies conducted in response to the clinical hold and remove any statements not supported by the data the Company generated. |
The FDA also requested that the Company address the following issues as an amendment to the Company’s IND:
| · | Provide a Certificate of Analysis for pc3/2B1 plasmid that includes tests for assessing purity, safety, and potency; |
| · | Perform qualification studies for the drug substance filling step to ensure that the Company’s product candidate for pancreatic cancer remains sterile and stable during the filling process; |
| · | Submit an updated batch analysis for the Company’s product candidate for the specific lot that will be used for manufacturing all future product candidates; |
| · | Provide additional details for the methodology for the Resorufin (CYP2B1) potency and the PrestoBlue cell metabolic assays; |
| · | Provide a few examples of common microcatheters that fit the specifications in the Company’s Angiography Procedure Manual; |
| · | Clarify the language in our Pharmacy Manual regarding proper use of the syringe fill with the Company’s product candidate for pancreatic cancer; and |
| · | Provide a discussion with data for trial of the potential for cellular and humoral immune reactivity against the heterologous rat CYP2B1 protein and potential for induction of autoimmune-mediated toxicities in our study population. |
The Company assembled a scientific and regulatory team of experts to address the FDA requests. That team has been working diligently to complete the items requested by the FDA. The Company is in the latter stages of conducting the studies and providing the information requested by the FDA.
| F-9 |
Impact of the COVID-19 Pandemic on the Company’s Operations
COVID-19 continues to cause uncertainty and significant, industry-wide delays in clinical trials. The availability of vaccines holds promise for the future; however, new variants of the virus and potential waning immunity from vaccines may result in continued impact from COVID-19 in the future, which could adversely impact our operations. Although the Company is not yet in a clinical trial, the Company has filed an IND with the FDA to commence a clinical trial in LAPC. While the IND has been placed on clinical hold by the FDA, the Company has assessed the impact of COVID-19 on its operations.
Many clinical trials have been delayed due to COVID-19. There are numerous reasons for these delays. For example, patients have shown a reluctance to enroll or continue in a clinical trial due to fear of exposure to COVID-19 when they are in a hospital or doctor’s office. There are local, regional and state-wide orders and regulations restricting usual normal activity by people. These discourage and interfere with patient visits to a doctor’s office if the visit is not COVID-19 related. Healthcare providers and health systems have shifted their resources away from clinical trials toward the care of COVID-19 patients. The FDA and other healthcare providers are making product candidates for the treatment of COVID-19 a priority over product candidates unrelated to COVID-19.
As a result of COVID-19 and the mitigation efforts to address it, the Company may experience additional disruptions that could adversely impact its business and clinical trial, if allowed to proceed, including: (i) delays or difficulties in enrolling patients in the Company’s Phase 2b clinical trial if the FDA allows the Company to go forward with the trial; (ii) delays or difficulties in clinical site activation, including difficulties in recruiting clinical site investigators and clinical site personnel; (iii) delays in clinical sites receiving the supplies and materials needed to conduct the clinical trial, including interruption in global shipping that may affect the transport of the Company’s clinical trial product; (iv) changes in local regulations as part of a response to COVID-19 which may require the Company to change the ways in which its clinical trial is to be conducted, which may result in unexpected costs, or to discontinue the clinical trial altogether; (v) diversion of healthcare resources away from the conduct of clinical trials, including the diversion of hospitals serving as the Company’s clinical trial sites and hospital staff supporting the conduct of the Company’s clinical trial; (vi) interruption of key clinical trial activities, such as clinical trial site monitoring, due to limitations on travel imposed or recommended by federal or state governments, employers and others, or interruption of clinical trial subject visits and study procedures, the occurrence of which could affect the integrity of clinical trial data; (vii) risk that participants enrolled in our clinical trials will acquire COVID-19 while the clinical trial is ongoing, which could impact the results of the clinical trial, including by increasing the number of observed adverse events; (viii) delays in necessary interactions with local regulators, ethics committees, and other important agencies and contractors due to limitations in employee resources or forced furlough of government employees; (ix) limitations in employee resources that would otherwise be focused on the conduct of the Company’s clinical trial because of sickness of employees or their families or the desire of employees to avoid contact with large groups of people; (x) refusal of the FDA to accept data from clinical trials in affected geographies; and (xi) interruption or delays to the Company’s clinical trial activities.
As a result of COVID-19, commencement of the Company’s clinical trial to treat LAPC may be delayed beyond the lifting of the clinical hold by the FDA should that occur. Also, enrollment may be difficult for the reasons discussed above. In addition, after enrollment in the trial, if patients contract COVID-19 during their participation in the trial or are subject to isolation or shelter in place restrictions, this may cause them to drop out of our clinical trial, miss scheduled therapy appointments or follow-up visits or otherwise fail to follow the clinical trial protocol. If patients are unable to follow the clinical trial protocol or if the trial results are otherwise affected by the consequences of COVID-19 on patient participation or actions taken to mitigate COVID-19 spread, the integrity of data from the clinical trial may be compromised or not be accepted by the FDA. This could further adversely impact or delay the Company’s clinical development program if the FDA allows it to proceed.
Clinical trials in the biopharma industry may be delayed due to COVID-19. There are numerous reasons for these potential delays. The impact relates to delays in: (i) completing studies required by the FDA; (ii) manufacturing a new batch of CypCap™ for the Company’s planned clinical trial in LAPC; (iii) manufacturing syringes of CypCaps™ for some of the Company’s preclinical studies to be completed and for use in the Company’s Malignant Ascites Program; and (iv) securing third party contractors to conduct various R&D projects for the Company. As a result, there may be delays in generating responses to the requests from the FDA related to the clinical hold. Many of these potential delays are also due to the impact of COVID-19 in foreign countries where the Company is conducting these preclinical studies, including India, Europe, Singapore and Thailand. There have also been supply chain interruptions due to COVID-19.
It is highly speculative in projecting the effects of COVID-19 on the Company’s proposed clinical development program and the Company generally. Moreover, the various precautionary measures taken by many governmental authorities around the world in order to limit the spread of COVID-19 has had and may continue to have an adverse effect on the global markets and global economy, including on the availability and pricing of employees, resources, materials, manufacturing and delivery efforts and other aspects of the global economy. The continuation of COVID-19 could materially disrupt the Company’s business and operations, hamper its ability to raise additional funds or sell securities, continue to slow down the overall economy, curtail consumer spending, interrupt the Company’s sources of supply, and make it hard to adequately staff the Company’s operations. The effects of COVID-19 quickly and dramatically change over time. Its evolution is difficult to predict, and no one is able to say with certainty when the pandemic will cease to have an impact on the Company’s operations.
| F-10 |
Company Background
The Company is a Nevada corporation incorporated in 1996. In 2013, the Company restructured its operations to focus on biotechnology. The restructuring resulted in the Company focusing all its efforts upon the development of a novel, effective and safe way to treat cancer and diabetes. In January 2015, the Company changed its name from Nuvilex, Inc. to PharmaCyte Biotech, Inc. to reflect the nature of its current business. In October 2021, the Company moved its headquarters to Las Vegas, Nevada.
Nasdaq Listing
The Company’s common stock began trading on Nasdaq on August 10, 2021, under the symbol “PMCB.” Prior to that, the Company’s common stock was quoted on the OTCQB Market under the symbol “PMCB.” Following the reverse stock split (discussed below) of the Company’s common stock on July 12, 2021, and until August 6, 2021, the OTCQB Market Symbol for the Company’s common stock had been “PMCBD.” Thereafter, it reverted to “PMCB.”
Reverse Stock Split
Effective July 12, 2021, the Company filed a Certificate
of Change with the Nevada Secretary of State that authorized a
NOTE 2 – SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES
Principles of Consolidation and Basis of Presentation
The Consolidated Financial Statements include
the accounts of the Company and its wholly owned subsidiaries. The Company operates independently and through four wholly owned subsidiaries:
(i) Bio Blue Bird; (ii) PharmaCyte Biotech Europe Limited; (iii) PharmaCyte Biotech Australia Pty. Ltd.; and (iv) Viridis Biotech, Inc.
and are prepared in accordance with U.S. GAAP and the Rules and Regulations of the Commission. Upon consolidation, intercompany balances
and transactions are eliminated. The Company’s
Use of Estimates in the Preparation of Financial Statements
The preparation of financial statements in accordance with U.S. GAAP requires the use of estimates and assumptions that affect the reported amounts of assets and liabilities, disclosure of contingent assets and liabilities known to exist as of the date the financial statements are published and the reported amounts of revenues and expenses during the reporting period. Uncertainties with respect to such estimates and assumptions are inherent in the preparation of the Company’s consolidated financial statements; accordingly, it is possible that the actual results could differ from these estimates and assumptions, which could have a material effect on the reported amounts of the Company’s consolidated financial position and results of operations. The severity, magnitude and duration, as well as the economic consequences of COVID-19, are uncertain, rapidly changing and difficult to predict. Therefore, the Company’s accounting estimates and assumptions may change over time in response to COVID-19 and may change materially in future periods.
Cash and Cash Equivalents
Cash and cash equivalents include cash in banks and short-term liquid investments purchased with maturities of three months or less.
| F-11 |
Intangible Assets
The Financial Accounting Standards Board (“FASB”) standard on goodwill and other intangible assets prescribes a two-step process for impairment testing of goodwill and indefinite-lived intangibles, which is performed annually, as well as when an event triggering impairment may have occurred. The first step tests for impairment, while the second step, if necessary, measures the impairment. The Company has elected to perform its annual analysis at the end of its reporting year.
The Company’s intangible assets are licensing
agreements related to the Cell-in-a-Box® technology for $
These intangible assets have an indefinite life; therefore, they are not amortizable.
The Company concluded that there was
Impairment of Long-Lived Assets
The Company evaluates long-lived assets for impairment whenever events or changes in circumstances indicate that the carrying value of an asset may not be fully recoverable. If the estimated future cash flows (undiscounted and without interest charges) from the use of an asset are less than carrying value, a write-down would be recorded to reduce the related asset to its estimated fair value. No impairment was identified or recorded during the years ended April 30, 2022, and 2021.
Fair Value of Financial Instruments
For certain of the Company’s non-derivative financial instruments, including cash, accounts payable and accrued expenses, the carrying amount approximates fair value due to the short-term maturities of these instruments.
Accounting Standards Codification (“ASC”) Topic 820, “Fair Value Measurements and Disclosures,” requires disclosure of the fair value of financial instruments held by the Company. ASC Topic 825, “Financial Instruments,” defines fair value, and establishes a three-level valuation hierarchy for disclosures of fair value measurement that enhances disclosure requirements for fair value measures. The carrying amounts reported in the consolidated balance sheets for current liabilities qualify as financial instruments and are a reasonable estimate of their fair values because of the short period between the origination of such instruments and their expected realization and their current market rate of interest. The three levels of valuation hierarchy are defined as follows:
| · | Level 1. Observable inputs such as quoted prices in active markets; |
| · | Level 2. Inputs, other than the quoted prices in active markets, which are observable either directly or indirectly; and |
| · | Level 3. Unobservable inputs in which there is little or no market data, which require the reporting entity to develop its own assumptions. |
Income Taxes
Deferred taxes are calculated using the liability method whereby deferred tax assets are recognized for deductible temporary differences and operating loss and tax credit carry forwards, and deferred tax liabilities are recognized for taxable temporary differences. Temporary differences are the differences between the reported amounts of assets and liabilities and their tax bases. Deferred tax assets are reduced by a valuation allowance when, in the opinion of management, it is more likely than not that some portion or all the deferred tax assets will not be realized. Deferred tax assets and liabilities are adjusted for the effects of changes in tax laws and rates on the date of enactment.
| F-12 |
A valuation allowance is provided for deferred income tax assets when, in management’s judgment, based upon currently available information and other factors, it is more likely than not that all or a portion of such deferred income tax assets will not be realized. The determination of the need for a valuation allowance is based on an on-going evaluation of current information including, among other things, historical operating results, estimates of future earnings in different taxing jurisdictions and the expected timing of the reversals of temporary differences. The Company believes the determination to record a valuation allowance to reduce a deferred income tax asset is a significant accounting estimate because it is based on, among other things, an estimate of future taxable income in the U.S. and certain other jurisdictions, which is susceptible to change and may or may not occur, and because the impact of adjusting a valuation allowance may be material. In determining when to release the valuation allowance established against the Company’s net deferred income tax assets, the Company considers all available evidence, both positive and negative. Consistent with the Company’s policy, and because of the Company’s history of operating losses, the Company does not currently recognize the benefit of all its deferred tax assets, including tax loss carry forwards, which may be used to offset future taxable income. The Company continually assesses its ability to generate sufficient taxable income during future periods in which deferred tax assets may be realized. When the Company believes it is more likely than not that it will recover its deferred tax assets, the Company will reverse the valuation allowance as an income tax benefit in the statements of operations.
The U.S. GAAP method of accounting for uncertain tax positions utilizes a two-step approach to evaluate tax positions. Step one, recognition, requires evaluation of the tax position to determine if based solely on technical merits it is more likely than not to be sustained upon examination. Step two, measurement, is addressed only if a position is more likely than not to be sustained. In step two, the tax benefit is measured as the largest amount of benefit, determined on a cumulative probability basis, which is more likely than not to be realized upon ultimate settlement with tax authorities. If a position does not meet the more likely than not threshold for recognition in step one, no benefit is recorded until the first subsequent period in which the more likely than not standard is met, the issue is resolved with the taxing authorities or the statute of limitations expires. Positions previously recognized are derecognized when the Company subsequently determines the position no longer is more likely than not to be sustained. Evaluation of tax positions, their technical merits and measurements using cumulative probability are highly subjective management estimates. Actual results could differ materially from these estimates.
On March 27, 2020, Congress enacted the Coronavirus Aid, Relief and Economic Security ("CARES") Act to provide certain relief as a result of the Coronavirus Disease 2019 outbreak. The Company maintains a full valuation allowance on its U.S. net deferred tax assets. Deferred tax asset remeasurement (tax expense) was offset by a net decrease in valuation allowance, which resulted in no impact on the Company's income tax expense. Therefore, the Company does not expect the provisions in the CARES Act will impact the Company’s consolidated financial statements.
On March 11, 2021, Congress enacted the American Rescue Plan Act of 2021, the Company does not expect the provisions of this Act will impact the Company’s consolidated financial statements.
Research and Development
Research and development expenses consist of costs incurred for direct and overhead-related research expenses and are expensed as incurred. Costs to acquire technologies, including licenses, which are utilized in research and development and that have no alternative future use are expensed when incurred. Technology developed for use in the Company’s product candidates is expensed as incurred until technological feasibility has been established.
R&D costs for the years ended April 30, 2022,
and 2021 were $
The Company recognizes stock-based compensation expense for only those awards ultimately expected to vest on a straight-line basis over the requisite service period of the award. The Company estimates the fair value of stock options using a Black-Scholes-Merton valuation model. This model requires the input of highly subjective assumptions, including the option's expected term and stock price volatility. In addition, judgment is also required in estimating the number of stock-based awards that are expected to be forfeited. Forfeitures are estimated based on historical experience at the time of grant and revised, if necessary, in subsequent periods if actual forfeitures differ from those estimates. The assumptions used in calculating the fair value of share-based payment awards represent management's best estimates, but these estimates involve inherent uncertainties and the application of management's judgment. Thus, if factors change and the Company uses different assumptions, the stock-based compensation expense could be materially different in the future.
| F-13 |
Concentration of Credit Risk
The Company has no significant off-balance-sheet
concentrations of credit risk such as foreign exchange contracts, options contracts or other foreign hedging arrangements. The Company
maintains most of its cash balance at a financial institution located in California. Accounts at this institution are insured by the Federal
Deposit Insurance Corporation up to $250,000. Uninsured balances aggregated approximately $
Foreign Currency Translation
The Company translates the financial statements of its foreign subsidiaries from the local (functional) currencies to U.S. dollars in accordance with FASB ASC 830, Foreign Currency Matters. All assets and liabilities of the Company’s foreign subsidiaries are translated at year-end exchange rates, while revenue and expenses are translated at average exchange rates prevailing during the year. Adjustments for foreign currency translation fluctuations are excluded from net loss and are included in other comprehensive income (loss). Gains and losses on short-term intercompany foreign currency transactions are recognized as incurred.
NOTE 3 – ACCRUED EXPENSES
Accrued expenses at April 30, 2022, and 2021, are summarized below:
| 2022 | 2021 | |||||||
| Payroll related costs | $ | $ | ||||||
| R&D costs | ||||||||
| Director and Officer insurance financing | ||||||||
| Other | ||||||||
| Total | $ | $ | ||||||
The Director and Officer Insurance Policy for
the policy term of September 8, 2021, through September 8, 2022, was paid in full on August 8, 2021. The Company financed the Director
and Officer Insurance Policy for the policy term of March 8, 2021, through September 8, 2021. The financing agreement had an interest
rate of
NOTE 4 – SMALL BUSINESS ADMINISTRATION – PAYCHECK PROTECTION PROGRAM
On March 27, 2020, the CARES Act was enacted to
provide financial aid to family and businesses impacted by COVID-19. The Company participated in the CARES Act, and on April 15,
2020, the Company entered into a note payable with a bank under the Small Business Administration (“SBA”), Paycheck Protection
Program (“PPP”) in the amount of $
The Company used the proceeds from the PPP loan
for qualifying expenses as defined in the PPP. The Company also applied for forgiveness of the PPP loan in accordance with the terms of
the CARES Act. The SBA issued a notice of PPP loan forgiveness with an effective date of April 28, 2021, forgiving the entire principal
of $
| F-14 |
NOTE 5 – COMMON STOCK TRANSACTIONS
A summary of the Company’s compensatory stock activity and related weighted average grant date fair value information for the years ended April 30, 2022, and 2021, are as follows:
In January 2020, the Company awarded shares of common stock to the executive officers of the Company as part of their compensation agreements for 2020. These shares vest monthly over a twelve-month period and are subject to them continuing service under the agreements. During the years ended April 30, 2022, and 2021, the Company recorded a non-cash compensation expense in the amount of $and $, respectively. There were unvested shares as of April 30, 2022, and 2021, respectively.
During the year ended April 30, 2021, four non-employee members of the Board were issued shares of common stock pursuant to their Director Letter Agreements (“DLAs”) in respect of their service during that year. The shares were fully vested upon issuance. The Company recorded a non-cash expense of $and $for the years ended April 30, 2022, and 2021, respectively. There were unvested shares remaining related to such DLAs as of April 30, 2022, and 2021.
During the year ended April 30, 2021, four consultants were issued shares of common stock pursuant to their consulting agreements with the Company. The shares vest monthly over a twelve-month period and are subject to the consultants continuing to provide services under their consulting agreements. The Company recorded a non-cash consulting expense in the amount of $and $for the years ended April 30, 2022, and 2021, respectively. There were unvested shares remaining related to these consulting agreements as of April 30, 2022, and 2021.
During the year ended April 30, 2021, a consultant was issued shares of common stock in respect of his services as the Chairman of the Company’s Medical and Scientific Advisory Board with vesting subject to the consultant continuing to provide services to the Company. The Company recorded a non-cash consulting expense in the amount of $and $for the years ended April 30, 2022, and 2021, respectively. There were unvested shares remaining related to his compensation arrangement as of April 30, 2022, and 2021.
In January 2021, the Company awarded shares of common stock to the executive officers of the Company as part of their compensation agreements for 2021. These shares vest monthly over a twelve-month period and are subject to the executive officers continuing to provide service under their compensation agreements. During the years ended April 30, 2022, and 2021, the Company recorded a non-cash compensation expense in the amounts of $and $, respectively. There were and unvested shares as of April 30, 2022, and 2021, respectively.
During the year ended April 30, 2022, four non-employee members of the Board were issued shares of common stock pursuant to their DLAs in respect of their service during that year. The shares were fully vested upon issuance. The Company recorded a non-cash expense of $ for the year ended April 30, 2022. There were unvested shares remaining related to such DLAs as of April 30, 2022, and 2021.
During the year ended April 30, 2022, four consultants were issued shares of common stock pursuant to their consulting agreements with the Company. The shares vest monthly over a twelve-month period and are subject to the consultants continuing to provide services under their consulting agreements. The Company recorded a non-cash consulting expense in the amount of $for the year ended April 30, 2022. There were unvested shares remaining related to these consulting agreements as of April 30, 2022.
During the year ended April 30, 2022, a consultant was issued shares of common stock in respect of his services as the Chairman of the Company’s Medical and Scientific Advisory Board with vesting subject to the consultant continuing to provide services to the Company. The Company recorded a non-cash consulting expense in the amount of $for the year ended April 30, 2022. There were unvested shares remaining related to his compensation arrangement as of April 30, 2022.
In January 2022, the Company awarded shares of common stock to the executive officers of the Company as part of their compensation agreements for 2022. These shares vest monthly over a twelve-month period and are subject to the executive officers continuing to provide service under their compensation agreements. During the year ended April 30, 2022, the Company recorded a non-cash compensation expense in the amounts of $. There were unvested shares as of April 30, 2022.
On March 1, 2021, the Company received notices
of cashless exercises of 26 warrant agreements. The cashless exercises resulted in the issuance of
| F-15 |
All shares were issued without registration under the Securities Act in reliance upon the exemption afforded by Section 4(a)(2) of the Securities Act.
On September 28, 2017, an S-3 Registration
Statement (“Second S-3”) was declared effective by the Commission for the Company to sell from time to time in one or more
public offerings of up to $50 million of its securities on a “shelf offering” basis. During the year ended April 30, 2021,
the Company sold and issued approximately shares of common stock, at prices ranging from approximately $15 to $45 per share. Net
of underwriting discounts, legal, accounting, and other offering expenses, the Company received proceeds of approximately $
A summary of the Company’s non-vested restricted stock activity and related weighted average grant date fair value information for the last two years ended April 30, 2022, are as follows:
| Shares | Weighted Average Grant Date Fair Value | |||||||
| Unvested, at April 30, 2020 | ||||||||
| Granted | ||||||||
| Vested | ( | ) | ||||||
| Expired | ||||||||
| Unvested, at April 30, 2021 | ||||||||
| Granted | ||||||||
| Vested | ( | ) | ||||||
| Expired | ||||||||
| Unvested, at April 30, 2022 | $ | |||||||
2021 Equity Incentive Plan
Effective June 30, 2021, the Company implemented the 2021 Equity Incentive Plan (“2021 Equity Plan”) as approved by the Company’s stockholders. The 2021 Equity Plan is administered by the Compensation Committee of the Board and has shares available under this plan. The 2021 Equity Plan can issue various types of awards, as follows: stock options, stock appreciation rights, restricted stock, restricted stock units, and cash or other stock-based awards. The 2021 Equity Plan is available to be issued to employees, directors, consultants, and other individuals who provide services to the Company. An incentive stock options (“ISOs”) can only be granted to employees and shall not exceed 10-years (5-years in the case of ISOs granted to any 10% shareholder).
Stock Options
As of April 30, 2022, the Company had outstanding stock options to its directors and officers (collectively, “Employee Options”) and consultants (“Non-Employee Options”).
During the years ended April 30, 2022, and 2021, the Company granted and Employee Options, respectively.
The fair value of the Employee Options at the date of grant was estimated using the Black-Scholes-Merton option-pricing model, based on the following weighted average assumptions:
| Years Ended April 30, | ||||||||
| 2022 | 2021 | |||||||
| Risk-free interest rate | % | % | ||||||
| Expected volatility | % | % | ||||||
| Expected lives (years) | ||||||||
| Expected dividend yield | % | % | ||||||
| F-16 |
The Company’s computation of expected volatility is based on the historical daily volatility of its publicly traded stock. For stock option grants issued during the years ended April 30, 2022, and 2021, the Company used a calculated volatility for each grant. The Company lacks adequate information about the exercise behavior now and has determined the expected term assumption under the simplified method provided for under ASC 718, which averages the contractual term of the Company’s stock options of five years with the average vesting term of two and one-half years for an average of three years. The dividend yield assumption of zero is based upon the fact the Company has never paid cash dividends and presently has no intention of paying cash dividends. The risk-free interest rate used for each grant is equal to the U.S. Treasury rates in effect at the time of the grant for instruments with a similar expected life.
During the years ended April 30, 2022, and 2021, the Company granted Non-Employee Options.
A summary of the Company’s stock option activity and related information for the two years ended April 30, 2022 are shown below:
| Options | Weighted Average Exercise Price per Share | Weighted Average Grant Date Fair Value per Share | ||||||||||
| Outstanding, April 30, 2020 | $ | $ | ||||||||||
| Issued | ||||||||||||
| Forfeited | ( | ) | ||||||||||
| Outstanding, April 30, 2021 | ||||||||||||
| Issued | ||||||||||||
| Forfeited | ( | ) | ||||||||||
| Outstanding, April 30, 2022 | $ | $ | ||||||||||
| Exercisable, April 30, 2022 | $ | $ | – | |||||||||
| Vested and expected to vest | $ | $ | – | |||||||||
A summary of the activity for unvested stock options during the years ended April 30, 2022, and 2021 is as follows:
| Options | Weighted Average Grant Date Fair Value per Share | |||||||
| Unvested, April 30, 2020 | $ | |||||||
| Issued | ||||||||
| Vested | ( | ) | ||||||
| Forfeited | ||||||||
| Unvested, April 30, 2021 | ||||||||
| Issued | ||||||||
| Vested | ( | ) | ||||||
| Forfeited | ||||||||
| Unvested, April 30, 2022 | $ | |||||||
| F-17 |
The Company recorded $and $of stock-based compensation related to the issuance of Employee Options to certain officers and directors in exchange for services during the years ended April 30, 2022, and 2021, respectively. At April 30, 2022, there remained $of unrecognized compensation expense related to unvested Employee Options granted to officers and directors, to be recognized as expense over a weighted-average period of the remaining eight months in the calendar year. The unvested options vest at 500 shares per month and are expected to be fully vested on December 31, 2022.
The following table summarizes the outstanding stock options by exercise price at April 30, 2022:
| Exercise Price | Number of Options Outstanding |
Weighted Average Remaining Contractual Life (Years) of Outstanding Options |
Weighted Average Exercisable Price Per Share |
Number of Options Exercisable |
Weighted Average Exercise Price Per Share of Exercisable Options |
|||||||||||||||||
| $ | 87.00 | $ | $ | |||||||||||||||||||
| $ | 109.35 | $ | $ | |||||||||||||||||||
| $ | 133.50 | $ | $ | |||||||||||||||||||
| $ | 82.95 | $ | $ | |||||||||||||||||||
| $ | 83.70 | $ | $ | |||||||||||||||||||
| $ | 80.10 | $ | $ | |||||||||||||||||||
| $ | 80.85 | $ | $ | |||||||||||||||||||
| $ | 102.45 | $ | $ | |||||||||||||||||||
| $ | 97.35 | $ | $ | |||||||||||||||||||
| $ | 74.25 | $ | $ | |||||||||||||||||||
| $ | 57.00 | $ | $ | |||||||||||||||||||
| $ | 60.60 | $ | $ | |||||||||||||||||||
| $ | 55.50 | $ | $ | |||||||||||||||||||
| $ | 51.00 | $ | $ | |||||||||||||||||||
| $ | 61.20 | $ | $ | |||||||||||||||||||
| $ | 36.00 | $ | $ | |||||||||||||||||||
| $ | 37.05 | $ | $ | |||||||||||||||||||
| $ | 15.75 | $ | $ | |||||||||||||||||||
| $ | 10.05 | $ | $ | |||||||||||||||||||
| $ | 26.55 | $ | $ | |||||||||||||||||||
| $ | 16.20 | $ | $ | |||||||||||||||||||
| $ | 3.19 | $ | $ | |||||||||||||||||||
| $ | 2.50 | $ | $ | |||||||||||||||||||
| Total | $ | $ | ||||||||||||||||||||
The aggregate intrinsic value of outstanding options as of April 30, 2022, was $. This represents options whose exercise price was less than the closing fair market value of the Company’s common stock on April 30, 2022, of approximately $ per share.
| F-18 |
Warrants
The warrants issued by the Company are equity classified. The fair value of the warrants was recorded as additional paid-in-capital, and no further adjustments are made.
The Company concluded the following warrants met the permanent equity criteria classification as they are freestanding financial instruments that are legally detachable and separately exercisable from the shares of common stock with which they were issued. The warrants are immediately exercisable and do not embody an obligation for the Company to repurchase the shares. The warrants also permit the holders to receive a fixed number of shares upon exercise and do not provide any guarantee of value or return.
The Company elected to early adopt ASU No. 2020-06 Debt - Debt with Conversion and Other Options (Subtopic 470-20) and Derivatives and Hedging — Contracts in Entity’s Own Equity (Subtopic 815-40) as of May 1, 2021. The early adoption of ASU No.2020-06 had an immaterial effect on the Company’s consolidated financial statements.
Effective August 12, 2021, the Company issued
Common Stock Warrant Agreements (“Common Warrants”) with respect to the First Offering. The Company issued Common Warrants
to purchase
Additionally, with respect to the First Offering,
the Company issued common stock warrant agreements to Wainwright (“Underwriter Warrants”) to purchase
Effective August 12, 2021, the Company issued
Effective August 23, 2021, the Company issued
additional Common Stock Warrant Agreements (“Series A Warrants”) with respect to its Registered Direct Public offering. The
Company issued Series A Warrants to purchase
Effective August 23, 2021, the Company
issued additional Common Stock Warrant Agreements (“Placement Agent Warrants”) with respect to its Registered Direct
Public Offering. The Company issued Placement Agent Warrants to purchase
Effective August 23, 2021, the Company issued
Pre-funded Warrants pursuant to the Registered Direct Offering to purchase
| F-19 |
In August 2021, the Company received
twenty-seven cash exercise notices relating to the Common Warrants with respect to the First Offering totaling
Series A Warrants and Placement Agent Warrants were issued pursuant to the Securities Purchase Agreement dated as of August 19, 2021. At the time, the Series A Warrants and the Placement Agent Warrants were issued, neither the Series A Warrants, the Placement Agent Warrants nor the underlying common stock was registered pursuant to the Securities Act. The Company registered the common stock underlying the Series A Warrants and the Placement Agent Warrants pursuant to a Registration Statement on Form S-3 (“Registration Statement”) filed with the Commission on November 8, 2021. The Registration Statement became effective on November 17, 2021.
A summary of the Company’s warrant activity and related information for the two years ended April 30, 2022, are shown below:
| Warrants | Weighted Per Share | |||||||
| Outstanding, April 30, 2020 | $ | |||||||
| Issued | ||||||||
| Exercised | ( | ) | ||||||
| Expired | ( | ) | ||||||
| Outstanding, April 30, 2021 | ||||||||
| Issued | ||||||||
| Exercised | ( | ) | ||||||
| Expired | ( | ) | ||||||
| Outstanding, April 30, 2022 | ||||||||
| Exercisable, April 30, 2022 | $ | |||||||
The following table summarizes additional information concerning warrants outstanding and exercisable at April 30, 2022:
| Exercise Prices | Number of Warrant Shares Exercisable at April 30, 2022 |
Weighted Average Remaining Contractual Life Years |
Weighted Average Exercise Price Per Share |
|||||||||
| $ | ||||||||||||
| $ | ||||||||||||
| $ | ||||||||||||
| $ | ||||||||||||
| $ | ||||||||||||
| $ | ||||||||||||
| $ | – | |||||||||||
| $ | ||||||||||||
NOTE 7 – LEGAL PROCEEDINGS
The Company is not currently a party to any pending legal proceedings, material or otherwise. There are no legal proceedings to which any property of the Company is subject.
| F-20 |
NOTE 8 – RELATED PARTY TRANSACTIONS
The Company had the following related party transactions during the years ended April 30, 2022, and 2021, respectively.
The Company owns
In April 2014, the Company entered the Vin-de-Bona
Consulting Agreement pursuant to which it agreed to provide professional consulting services to the Company. Vin-de-Bona is owned by Prof.
Günzburg and Dr. Salmons, both of whom are involved in numerous aspects of the Company’s scientific endeavors relating to cancer
and diabetes (Prof. Gunzburg is the Chairman of Austrianova, and Dr. Salmons is the Chief Executive Officer and President of Austrianova).
The term of the agreement is for 12 months, automatically renewable for successive 12-month terms. After the initial term, either party
can terminate the agreement by giving the other party 30 days’ written notice before the effective date of termination. The agreement
has been automatically renewed annually. The amounts incurred for the years ended April 30, 2022, and 2021, were approximately $
NOTE 9 – COMMITMENTS AND CONTINGENCIES
The Company acquires assets still in development and enters R&D arrangements with third parties that often require milestone and royalty payments to the third-party contingent upon the occurrence of certain future events linked to the success of the asset in development. Milestone payments may be required, contingent upon the successful achievement of an important point in the development lifecycle of the pharmaceutical product (e.g., approval of the product for marketing by a regulatory agency). If required by the license agreements, the Company may have to make royalty payments based upon a percentage of the sales of the pharmaceutical products if regulatory approval for marketing is obtained.
Office Lease
In May 2019, the Company entered into a lease for its office space in Laguna Hills, California for a one-year lease for the leased premises. The term of the lease expired on August 31, 2020.
On May 28, 2020, the Company entered into an additional six-month lease of this office space, commencing on September 1, 2020. The term of the new lease expired on February 28, 2021.
On May 24, 2021, the Company entered into an additional six-month lease of this office space, commencing on September 1, 2021, which expires on February 28, 2022.
In October 2021, the Company moved the Company’s headquarter from Laguna Hills, California to Las Vegas. Nevada. In doing so, the Company entered into a lease for office space in Las Vegas, Nevada. The term of the lease expires on April 30, 2022.
In January 2022, the Company entered into an additional six-month lease of the Las Vegas, Nevada office space, commencing on May 1, 2022, which expires on October 31, 2022.
Rent expenses for these offices for the years
ended April 30, 2022, and 2021, were $
The following table summarizes the Company’s aggregate future minimum lease payments required under the operating lease as of:
| Year Ending April 30, | Amount | |||
| 2023 | $ | |||
| $ | ||||
| F-21 |
Material Agreements
The Company’s material agreements are identified and summarized in Note 1 – Nature of Business – Company Background.
Compensation Agreements
The Company entered into executive compensation agreements with its three executive officers in March 2015, each of which was amended in December 2015 and March 2017. Each agreement has a term of two years with annual extensions thereafter unless the Company or the officer provides written notification of termination at least ninety days prior to the end of the term or subsequent extensions. The Company also entered a compensation agreement with a Board member in April 2015 which continued in effect until amended in May 2017.
The Company entered into amended and restated executive compensation agreements with two executive officers with an effective date of January 1, 2022 (“Amendment Date”). Each agreement has a term of three (3) years from the Amendment Date (“Initial Term”) and has automatic renewals of one (1) year (“Renewal Term”) unless the Company or the officer provides written notice of termination at least ninety (90) days prior to the end of the Initial Term or the Renewal Term.
In May 2017, the Company amended the compensation agreement with the Board members and the terms continue in effect until a member is no longer on the Board.
The Company has four independent directors. Each director receives the same compensation: (i) $12,500 in cash for each calendar quarter of service on the Board; (ii) 333 fully paid, non-assessable shares of the Company’s restricted common stock (“Shares”) annually; and (iii) a five-year option to purchase 333 Shares annually at an exercise price equal to the fair market value of the Shares on the date of grant. The Shares and the option Shares fully vest on the date of the grants.
NOTE 10 - INCOME TAXES
At April 30, 2022, the Company had federal
and state net operating loss carryforwards of approximately $
Current tax laws limit the amount of loss available to be offset against future taxable income when a substantial change in ownership occurs. Therefore, the amount available to offset future taxable income may be limited. Based on the assessment of all available evidence including, but not limited to, the Company’s limited operating history in its core business and lack of profitability, uncertainties of the commercial viability of its technology, the impact of government regulations and healthcare reform initiatives and other risks normally associated with biotechnology companies, the Company has concluded that is more likely than not that these operating loss carryforwards will not be realized. Accordingly, 100% of the deferred tax valuation allowance has been recorded against these assets.
Deferred income taxes reflect the net effect of temporary differences between the financial reporting carrying amounts of assets and liabilities and income tax carrying amounts of assets and liabilities. The components of the Company’s deferred tax assets and liabilities are as follows:
| April 30, | ||||||||
| 2022 | 2021 | |||||||
| Deferred tax assets: | ||||||||
| Net operating loss carryforwards | $ | |||||||
| Stock compensation | ||||||||
| Other | ||||||||
| Total deferred tax assets | ||||||||
| Valuation allowance | ( | ) | ( | ) | ||||
| Net deferred tax assets | $ | $ | ||||||
For all years presented, the Company did not recognize
any deferred tax assets or liabilities. The net change in valuation allowance for the years ended April 30, 2022, and 2021, was a decrease
of $
| F-22 |
The provision for income taxes differs from the provision computed by applying the Federal statutory rate to net loss before income taxes as follows:
| Years Ended April 30, | ||||||||
| 2022 | 2021 | |||||||
| Federal benefit at statutory rate | $ | ( | ) | ( | ) | |||
| State income taxes, net of Federal taxes | ( | ) | ( | ) | ||||
| Permanent differences | ||||||||
| Provision related to change in valuation allowance | ( | ) | ||||||
| Expired stock options | ||||||||
| Net valuation allowance for state tax deductions | ||||||||
| Other, net | ( | ) | ||||||
| Provision for income taxes | $ | $ | ||||||
There have been no changes to the Company’s liability for unrecognized tax benefits during the year ended April 30, 2022.
The Company files its income tax returns in the U.S. Federal jurisdiction and various state jurisdictions. As of the year ended April 30, 2022, the tax returns for 2016 through 2021 remain open to examination by the Internal Revenue Service and various state tax authorities.
The Company’s policy is to recognize any
interest and penalties related to unrecognized tax benefits as a component of income tax expense. As of the years ended April 30, 2022,
and 2021, the Company had accrued
Basic earnings (loss) per share is computed by dividing earnings available to common stockholders by the weighted average number of shares outstanding during the period. Diluted earnings per share is computed by dividing net income by the weighted average number of shares and potentially dilutive shares of common stock outstanding during the period increased to include the number of additional shares of common stock that would be outstanding if the potentially dilutive securities had been issued. Potential shares of common stock outstanding principally include stock options and warrants. During the years ended April 30, 2022, and 2021, the Company incurred losses. Accordingly, the effect of any common stock equivalent would be anti-dilutive during those periods and are not included in the calculation of diluted weighted average number of shares outstanding.
The table below sets forth the basic loss per share calculations:
| Years Ended April 30, | ||||||||
| 2022 | 2021 | |||||||
| Net loss | $ | ( |
) | $ | ( |
) | ||
| Basic weighted average number of shares outstanding | ||||||||
| Diluted weighted average number of shares outstanding | ||||||||
| Basic and diluted loss per share | $ | ( |
) | $ | ( |
) | ||
The table below sets forth these potentially dilutive securities:
| Years Ended April 30, | ||||||||
| 2022 | 2021 | |||||||
| Excluded options | ||||||||
| Excluded warrants | ||||||||
| Total excluded options and warrants | ||||||||
| F-23 |
NOTE 12 – PREFERRED STOCK
The Company has authorized shares of preferred stock, with a par value of $, of which one share has been designated as "Series A Preferred Stock". As of April 30, 2022, there are shares of preferred stock issued and outstanding.
The description of the Series A Preferred Stock below is qualified in its entirety by reference to the Company’s Articles of Incorporation, as amended.
The Series A Preferred Stock has the following features:
| · | There is one share of preferred stock designated as Series A Preferred Stock; | |
| · | The Series A Preferred Stock has a number of votes at any time equal to the number of votes then held by all other shareholders of the Company having a right to vote on any matter plus one. The Certificate of Designations that designated the terms of the Series A Preferred Stock cannot be amended without the consent of the holder of the Series A Preferred Stock; | |
| · | The Company may redeem the Series A Preferred Stock at any time for a redemption price of $1.00 paid to the holder of the share of Series A Preferred Stock; and | |
| · | The Series A Preferred Stock has no rights of transfer, conversion, dividends, preferences upon liquidation or participation in any distributions to shareholders. |
NOTE 13 – SUBSEQUENT EVENTS
In May 2022, the Board granted the Company’s Chief Executive Officer and Chief Financial Officer stock options of 529,000 and 201,860, respectively, and restricted stock units of 150,800 and 57,540, respectively. These grants were made subject to an increase in the Company’s authorized shares of common stock. The Company is planning to increase the authorized shares of common stock at its 2022 annual shareholders meeting.
In May 2022, the Board of Directors authorized a Share Repurchase Program whereby the Company would repurchase the Company’s common stock at the discretion of the Company’s Chief Executive Officer, depending on market conditions over a two-year period, in the amount of up to $10 million. The repurchases shall follow the applicable laws, including the Nevada Revised Statutes and Federal securities laws and in a manner to comply with the provisions of Rule 10b-18 under the Securities Act or any subsequent superseding or amending rule. As of July 28, 2022, there has been 851,981 shares of the Company’s common stock repurchased at an approximate cost of $2,091,000, including commissions.
On July 7, 2022, the Company received a notice of exercise relating to the Pre-funded Warrants pursuant to the registered direct offering in the amount of $880 which resulted in the issuance of 880,000 shares of common stock.
| F-24 |
PHARMACYTE BIOTECH, INC.
SCHEDULE II — VALUATION AND QUALIFYING ACCOUNTS
Years Ended April 30, 2022 and 2021
| Description | Balance at Beginning of Year |
Additions Charged to Costs and Expenses |
Charged to Other Accounts |
Deductions | Balance at End of Year |
|||||||||||||||
| Reserve Deducted in the Balance Sheets from the Asset to which it applies: | ||||||||||||||||||||
| Allowance for Deferred Tax Assets | ||||||||||||||||||||
| Year ended April 30, 2022 | $ | ( |
||||||||||||||||||
| Year ended April 30, 2021 | $ | |||||||||||||||||||
| F-25 |